| Ann. Medit. Burns Club - vol. VI - n. 2 - June 1993
A NEW PROGNOSTIC BURN INDEX Stavropoulou V., Daskalakis J., loannovich J. Centre of Plastic Surgery and Microsurgery, General State Hospital of Athens, Greece SUMMARY. 342 burned patients have been treated at the bums centre of our hospital during the last three years. An effort was made to examine the reliability of the usual bum indices and the Apache 11 severity score index, comparing their predicted mortality with the actual mortality in our sample. We concluded by forming a new prognostic index, which is more accurate in the prediction of mortality, because it considers objectively and in detail the patient's,general condition on admission. Introduction The importance of burn prognostic indices lies not only in the prediction of outcome of an individual patient, but also in the distribution of the patients in comparable groups of severity for therapeutic and research purposes. Although the prediction of the outcome of an individual patient is the first and main question of a patient's family, the quantitative measurement of a patient's illness using these indices is of great importance for the burn centre in deciding its therapeutic policy, evaluating new therapy and the quality of patient care, and estiffiatingthe cost of its services. The more accurate an index the more useful it is for this latter purpose. For this reason, nowadays, several burn indices based on different statistical methods are complicated and have been computerized in an effort to make them more accurate in their predictions. Nevertheless the most accurate prognosis in a Bums Centre is achieved either by using one of the known indices adapted to its particular needs and conditions or by producing its own new index and updating it continuously. Materials and methods 342 patients (140 female, 41%, and 202 male, 59%)
were studied, all admitted to the Bums Centre of the General State Hospital of Athens
during the period from July 1989 to July 1992. They suffered from thermal burns,
electrical and chemical burns being excluded. The distribution of the patients according
to age and to bum extent is given in Table 1 and Table 2. 315 patients (92.1%) presented
no inhalation bum although this was suspected in 52 of them. In these patients the
respiratory system was thoroughly examined. 7.9% of the patients had an inhalation bum
confirmed by clinical symptoms and abnormal blood gases. For 8 patients a respirator was
required. The mortality according to bum extent is given in Table 3. For the determination
of the survival rate we applied the usual burn indices (Fisher-Bull, Baux, BUS - UDB,
Stem, ABSI, Bowser, Roi, Clark), as well as the APACHE 11 severity index, which is used in
Intensive Care Units (ICU) for non burned patients suffering from single or multiple organ
system failure (Table 4). While some of these indices are empirical, others are based on
statistical methods such as logistic regression, probit analysis and discriminant
analysis. The parameters taken into account in the indices we used in our sample are shown
in Table 5. Clearly the bum indices include mainly empirical parameters; APACHE H however
also includes precise clinical and laboratory measurements. We used these indices as
reported by their authors, according to their instructions and restrictions, as follows-
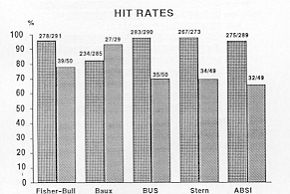
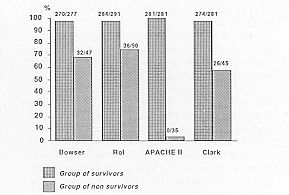
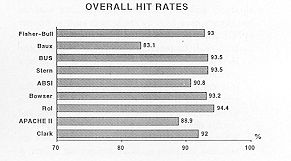
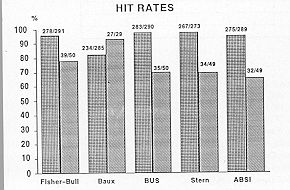
For the APACHE 11 index, after calculation of the z-score, we tried to find the probability of death using in the final equation the constants of multiple trauma, infection and sepsis. Results and discussion The calculated hit rates of the indices (Fig. 1) were generally elevated. Most of them had a high hit rate for survivors, but a low rate for non-survivors, except for the Baux index, which seems to be more accurate in predicting death. The most unreliable of them all, especially in predicting death, is APACHE 11, which underestimates the severity of bum injury even when calculated with the most unfavourable constant of sepsis. Probably there are two explanations for this. On the one hand this index neglects the extent and the depth of the burn, which are significant determinants of mortality. On the other hand, like all ICU indices, it is reliable in predicting the outcome of critically ill patients, but not the outcome of patients with chronic diseases. The overall hit rates of Baux and APACHE 11 indices were under 90% (Fig. 2).
The other indices had hit rates ranging from 90.8% to 94.4%. The hit rates given by the authors in their samples were considerably 'superior in their prediction of nonsurvivors than our hit rates, when the same indices were applied to our sample (Table 6). This phenomenon may be explained by the fact that these indices were applied on different samples and in centres with different treatment standards. We agree with other researchers that every burn centre must adapt an index to its particular conditions and update it continuously. We believe that the most accurate prognosis in a burn centre is achieved by using prospectively the index which has been produced there retrospectively. A new prognostic index (Vergina) For this reason we formed our own new prognostic index (Yergina). For the determination of mortality we used in the final equation those of the previously reported variables that were statistically significant for the outcome of the patient (Table 7). These variables can be classified in 3 groups. The first group includes general factors common to all burn indices, while the other two groups include variables which are affected by the pathophysiology of the burn and demonstrate the degree of haemoconcentration and the condition of the respiratory and renal function at the time of admission (Table 8). As known, any delay in the initiation of treatment influences these conditions as well as the outcome of the patient. A combination of all these variables was made in a predictive model, using discriminant analysis, and we developed an equation to discriminate between survivors and non-survivors. Discriminant analysis has already been used by researchers such as Bowser (1982), and it has the following advantages:
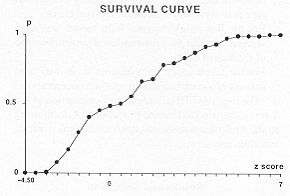
A score is derived from the multifactorial equation, which includes the 14 significant variables, appropriate coefficients and a constant. This is shown in Table 9. Once the z-score is calculated, reference to the survival curve (Fig. 3) predicts mortality.
Our results are shown in Table 10. The overall correct classification was 97. 1 % (Fig. 4).
The accuracy of the Vergina index is obvious, because of its high overall hit rate, but above all it is worth emphasizing its reliability for the prediction of death (hit rate 89.2%, the highest of all the proposed bum indices) (Fig. 5).
Conclusion The usual bum indices are sufficiently reliable but the Vergina index is more accurate in prediction of mortality in burns, because it considers objectively and in detail the patient's general condition at the time of admission. The predictive accuracy of the APACHE 11 index in bums is poor.
RESUME. Les auteurs ont traité 342 patients brûlés chez le centre des brûlés de leur hôpital pendant les trois dernières années. Ils se sont proposés d'examiner la fiabilité des plus communs indices des brûlures et l'indice de gravité Apache 11, en comparant la mortalité prédite par les indices avec la mortalité effective observée chez leurs patients. Ils concluent leur étude avec la proposition d'un nouvel indice pronostique qui est plus précis, pour ce qui concerne la prédiction de la mortalité, parce qu'il considère objectivement et d'une façon détaillée les conditions générales du patient au moment de l'hospitalisation. BIBLIOGRAPHY
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||