| Ann. Medit. Burns Club - vol. 6 - n. 2 - June 1993
COMPARATIVE STUDY OF SEPSIS IN BURN DURING THREE PERIODS OF
TIME
Herruzo-Cabrera R.,* Calle-Puffin E.,*
Garcia-Torres V.,** Luengo-Matos W, Lenguas-Portero F,*** Rey-Calero J.*
* DptO Medicina Preventiva y Salud Pùblica, Hospital
La Paz, Facultad de Medicina, Universidad Autèrioma de Madrid, Spain
** Dpto Cirurgia Plàstica y Reparadora, Hospital La Paz
*** Unidad de Cuidados Intensivos, Hospital La Paz
SUMMARY. A
comparative study was performed to investigate the variations in the septicaemia rate
occuring in the Critical Area of the Burn Unit in La Paz Hospital. Three time periods were
compared: 1980-84, 1985-86 and 1987-90, coinciding with major modifications in preventive
measures in bum patients. The analysis was made by direct standardization and multiple
logistic regression. Our results show that during the most recent time period the
incidence of septicaemia decreased significantly and that the decrease coincided with the
introduction of intensive decontamination treatment.
Introduction
Burn patient survival has improved
over the last 50 years, as a consequence of advances in bum management (1). The reduction
in mortality in a given period is due to the changes in treatment during that time (2, 3).
Hydric therapy has elin-finated hypovolaemic shock as the major cause of death; the
prevention and treatment of bum sepsis, which includes earlier surgical debridement, the
use of topical antibiotics and systemic antibiotherapy in patients with systemic or
urinary infection, etc., are factors that diminish the risk of microbial invasion and
septicaemia (4).
Despite the wide use of antibiotcs, infections caused by multiple agents such as Pseudomonas,
Staphylococcus aureus, E. coli, etc. are present in a large number of burn patients,
and if septicaemia occurs burn patient mortality is elevated (5). At present, sepsis and
its sequelae and respiratory complications are the most important causes of death in
serious bum patients.
Environmental control to reduce the number and character of micro-organisms is very
important in diminishing bum infections. Although the objective of strict isolation is to
eliminate exogenous sources of infection (6), it cannot eliminate endogenous sources,
particularly intestinal contamination. Endogenous sources can be direct, from the mouth or
anus, and by intestinal translocation, which increases the permeability of the intestinal
wall to micro-organisms from the lumen (7, 8, 9).
The prophylactic use of antibiotics to suppress colon flora, in addition to strict
isolation techniques (10), has considerably decreased the number of bum infections. This
joint effect is the theoretical basis for the establishment of selective intestinal
decontan-fination measures exclusively for intestinal pathogens (11), since the
indiscriminate use of antibiotics destroys intestinal microflora involved in host
resistance to infection (12).
Another classic infection source in Intensive Care Units is the catheter (13).
The present study evaluates all previous therapeutic measures, including a protocolized
treatment, called Intensive Burn Decontamination (IBD), which includes local and systemic
decontamination, as well as early debridement, avoidance of manipulations, etc.
The incidence of septicaemia morbidity has been studied and compared during three
different time periods, in our Burn Unit at La Paz Hospital.
Material and methods
All patients spending two or more
days in the Critical Area of the Burn Unit in La Paz Hospital from 1980 to 1990 were
studied.
The Bum Unit was a part of the Plastic Surgery, Department until 1985. In 1985, it became
a multidisciplinary unit served by the Plastic Surgery Service, the Intensive Medicine
Service and the Preventive Medicine Service.
The Critical Bum Unit has twelve single rooms.
There is a written protocol on the management of burn patients that is reviewed every two
years and published as a guide.
The major modifications that have prevented infection in bum patients were:
- beginning in 1985, surgical prophylaxis; pharyngeal
decontamination with hexetidine- spray; twice weekly microbiological monitorization;
- beginning in 1987, 1BD as follows: intestinal
decontamination with three drugs, usually tobramycin 300 mg/day plus cholymycin 400 mg/day
plus nystatin 100,000-150,000 U/Kg/day nasal decontamination with hexetidine and topical
treatment of the burn itself with clorhexidine 0.5% cream (14);
- beginning in 1988, a topical treatment with clorhexidine
0.5% cream was initiated at the site of catheter insertion.
Between 1980 and 1984, patients were
followed in a record kept by the plastic surgeons. Since 1985 this information has been
recorded by the Preventive Medicine Service, using the same protocol during the entire
period that the patient is in the Critical Burn Unit. The records contain information on
the variables sex, age, percentage of burned body surface, previous disease, type of burn,
etc., as well as data on manipulation, surgical treatment of the burns, treatment, burn
infections and aetiology of the infection.
Septicaemia was diagnosed following CDC criteria and measured by:
Accumulated Incidence (A.I.): number of infected patients x 100 divided by the total
number of patients spending two or more days in the Unit. The association between
infection and qualitative variables was calculated with the Chi square test, and the
association between infection and numerical variables was calculated with analysis of
variance or Student's T test.
Multivariant analysis was performed with multiple logistic regression to control
confounding factors. All variables that were significant in bivariant analysis were
included in the multiple logistic regression analysis as independent.
Standardization was made in two different ways:
- by the direct method (15), which compared the incidence of
septicaemia in the three periods with that of the first period;
- by individual probability estimation (16), which included
each patient's value in the logistic regression equation. The probability of septicaemia
during the first period was taken as the referent level.
Results
The characteristics of the
population are described in Table 1, for the different time period studied.
During the second and third periods the burns were significantly larger. The number of
patients with more than 30% BSA affected was high (over 30% of the total patient number).
During the period 1985-86 an increase in bum depth was observed, the number of subdermal
bums being higher than in the period 1987-89. These differences were not however
statistically significant.
Patients in the most recent period were older, they presented more severe bums and they
had a high percentage of previous diseases. the frequency of the different aetiological
agents. Septicaemia became less frequent during the study period, excluding fungal
infections, which did not occur during the first time period at all, and decreased in the
last period compared to the second period. The significant increase of Gram+ cocci different
from S. aureus coincided with the decrease in the presence of S. aureus.
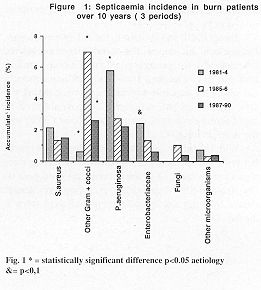
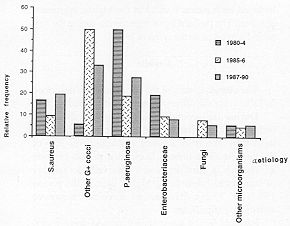
Figs. 1 and 2 show septicaemia frequency, and Tables III and IV refer to the A.I. of
septicaemia, i.e. the real incidence, the standardized incidence calculated by the
percentage of burned body surface, and the accumulated incidence of septicaemia calculated
by multiple logistic regression, taking the first period as the reference. The incidence
of septicaemia decreased during the second (30%) and the third period (60%).
With regards to septicaemia aetiology, differences between real incidence and estimated
incidence were significantly reduced in the second and third periods (by 50% and 85%
respectively), excepting septicaen-iias caused by fungi and Staphylococcus different from
S. aureus.
In general, the septicaemia percentage decreased during 1987-90 compared to 1985-86.
 |
 |
| Fig. 1* =
statistically significant difference p<0.05 aetiology &= p<0,1 |
Fig. 2: Septicaemia
aetiology in burn patients over 10 years (3 periods) |
|
Discussion
The incidence of septicaemia decreased
during the study period by about 51-60%, depending on the method of measurement and the
aetiological agents. The decrease was associated to the treatment used in each time
period. The reduction in the A.I. of sepsis for some aetiological agents, such as S. aureus,
P. aerugi . nosa and Enterobacteriaceae, which was 58% lower in the less
favourable situation, was marked. As we demonstrated in a previous paper (14), and in
agreement with the Manson study (11), intensive treatment decreases nasal and intestinal
colonization, which is the most important source of infection in the bum patient.
The number of non S. aureus isolated Gram+ cocci increased during 1985-86,
but this percentage decreased when clorhexidine 0.5% replaced argentic sulphadiazine in
topical bums therapy and the use of clorhexidine 0.5% cream was begun at the sites of
catheter insertion. However, we think that the increase in the number of Gram+ cocci
infections ' compared to 1980-84, was due to intensive therapy with parenteral feeding via
the central venous system.
The appearance of fungal septicaemia in the second time period, but not the first, was
probably due to the intensive therapy, which increased burn patient survival although
selecting some fungi (17). Fungal selection explains the large increase in fungal
septicaemia during the second study period and the decrease in its incidence, to one
quarter of the second study period value, in the third period, coinciding with 1BD.
Local and systemic decontamination, plus other treatment measures, such as surgical
debridement, frequent surgical interventions and prophylaxis at catheter insertion sites,
have significantly decreased the number of septicaemias in the Critical Bum Unit at our
Hospital.
DESCRIPTION OF
POPULATION
| STUDIED TIME PERIOD |
| |
80-84 |
85-86 |
87-90 |
| N' of Patients |
309 |
299 |
457 |
| Type of bum |
no % |
no % |
no % |
| Flame |
128
(41.8) |
122
(41.1) |
240
(52.5) |
| Scald |
89
(28.8) |
48 (16.2)* |
55
(12.0) |
| Electrical |
32
(10.3) |
36 (12.2) |
52
(11.4) |
| Chemical |
5
(1.6) |
9
(3.0) |
16
(3.5) |
| Explosion |
35
(11.3) |
19 (6.3) |
45
(10.5) |
| Other |
20
(6.5) |
63 (21.2)** |
46
(10.1)** |
| |
|
|
|
| Previous Disease |
|
|
|
| Epilepsy |
9
(2.9) |
11 (3.7) |
9
(2.0) |
| Neurological |
19 (9.2) |
14 (4.7) |
25
(4.9) |
| Heart |
8
(2.5) |
2
(0.7) |
8
(1.7) |
| Alcoholism |
5
(1.6) |
3
(1.0) |
22
(4.8)* |
| Drug abuse |
- - |
2
(0.7) |
10
(2.0) |
| Others |
83
(26.9) |
45 (15.1)* |
129
(28.3)** |
| No known prev. dis. |
185 (60.6) |
220
(74.1) |
254
(55.6)* |
| |
|
|
|
| Bum depth |
|
|
|
| Superficial |
128
(41.9) |
88 (29.6)* |
100
(21.9) |
| Deep |
103
(33.8) |
157 (52.9)* |
195
(42.7) |
| Subdermic |
74 (24.3) |
52 (17.5) |
161
(35.0)** |
| |
|
|
|
| % Burned Body surface |
13.5+
(0.9) |
21.9+
(1.3)** |
22.9+
(1. 1) |
| <10% |
171 (55.3) |
115 (39.9)** |
172
(39.3) |
| 10-30% |
103 (33.3) |
85 (29.5) |
128
(29.2) |
| >30% |
35 (11.3) |
88 (30.6)** |
138
(31.5) |
| |
|
|
|
| Mean Age |
37.2 1.1 |
38.1
1.1 |
42.9 1 |
| 1 st Debrid. (day) |
6.7
0,4 |
10.3
0.7 |
6.5 0.6** |
| last debrid. (day) |
16.6
0.9 |
14.6
0.9 |
15.7
1.5 |
| Operations per patient |
2.1 0.1 |
1.7
1.1 |
2.1
0.1 |
| Length of stay (days) |
23
1.2 |
13.5
0.8** |
16.7 0.8** |
| Parenteral feeding (%) |
41 (13.7%) |
83 (28%)* |
102 (22.3%) |
| Accumulated incidence
of septicaernias |
34 (11.0%) |
36 (12.2%) |
32
(7.4%)* |
|
| Table 1 |
|
STUDIED PERIODS |
|
80-84 |
85-86 |
87-90 |
| Real A.I. |
11% |
12% |
7.4% |
| A.I. by direct
standardization |
11% |
17.8% |
18.6% |
Estimated A.I. by
MLR standardization |
11% |
14.8% |
15.1% |
Changes in real A.I.
with regard to 1 st period* |
0% |
+10.9% |
-32.7% |
Changes in estimated
A.I.
by MLR standardization* |
0% |
-17.6% |
-51% |
|
| Table II |
|
| STUDIED PERIODS |
| |
80-84 |
85-86 |
87-90 |
| |
percentage real
incidence/estimated incidence |
| S. Aureus |
2.1 |
13/3.4 |
L5/3.6 |
| Gram+ Cocci (no S. aureus) |
0.6 |
7/0.97 |
2.6/1 |
| P. Aeruginosa |
5.8 |
2.7/9.4 |
2.2/9.8 |
| Enterobacterial |
2.4 |
13/3.9 |
0.6/4.1 |
| Fungi* |
0* |
1,10.2 |
0.4,10.2 |
| Others |
0.7 |
0.3,11.1 |
0.4/1.2 |
|
| Table III |
|
STUDIED
PERIODS |
| |
85-86 |
87-90 |
| S. Aureus |
-61.8% |
-58.3% |
| Gram+ Cocci (no S.
aureus) |
+521% |
+260% |
| P. Aeruginosa |
-71.3% |
-77.4% |
| Enterobacterial |
-66.7% |
-85.4% |
| Fungi |
+400% |
+100% |
| Others |
-72.3% |
-66.7% |
|
| Table IV |
|
RESUME. Les auteurs ont
effectué une étude comparative pour examiner les variations de la fréquence de la
septicémie qui s'est produite âa le secris cteur critique de l'Unité de Brûlures à
l'Hôpital La Paz. Ils ont confronté trois différentes périodes: 1980-84, 1985-86 et
1989-90, qui coïncidaient avec des modifications importantes dans les mesures
préventives chez les patients brûlés. L'analyse a été effectuée par la
standardisation directe et la régression logistique multiple. Les résultats démontrent
que pendant la période la plus récente la fréquence de la septicémie a diminué en %
en manière significative et que cette diminution a coïncidé avec l'introduction d'un
traitement intensif de décontamination.
BIBLIOGRAPHY
- Thompson P.B., Herndon D.N. Traber D.L. et al.: Effect
on mortality of inhalation injury. J. Trauma, 26: 63-9, 1986.
- Tompkins R.G., Burke J.F., Schoenfeld D.A. et al:. Prompt
scar excision: a treatment system contributing to reduced bum mortality. Ann. Surg., 128:
272-81, 1986.
- Dobke M.K., Simoni J., Ninneman J.L., Garret J., Dressel
L.: Postburn endotoxemia: effect of early excision on circulating endotoxin levels. Paper
presented at Annual Meeting, American Bum Association, Seattle, 1988.
- Herruzo-Cabrera R., Vizcaino-Alcaide M.J., Mayer R.F.,
Rey-Calero J.: A new in vitro model to test the effectiveness of topical antimicrobial
agents. Use of an artificial scar. Bums, 18: 35-8, 1992.
- Bang R.L., Saif J.K.: Mortality from bums in Kuwait. Bums,
15: 315-21, 1989.
- Settle J.A.D.: Infections in burns. J. Hosp. Infect, 6: 19,
1985.
- Carter E.A., Gonnella A., Tompkins R.G.: Increased
transcellular permeability of rat small intestine after thermal injury. Bums, 18: 117-20,
1992.
- Ziegler T.R., Smith R.J., O'Dwyer S.T. et al.: Increased
intestinal permeability associated with infection in burn patients. Arch. Surg., 123:
1313-7, 1988.
- Border J.R., Hasset J., La Duca J. et al.: The gut origin
septic states in blunt multiple trauma (ISS=40) in the ICU. Ann. Surg., 206: 427-48, 1987.
- Jarret F., Balish E., Moylan J.A. et al.: Clinical
experience with prophylactic antibiotic bowel suppression in burn patients. Surgery, 83:
523, 1978.
- Manson W.L., Klasen H.J., Sauer E.W., Olieman A.: Selective
intestinal decontamination for prevention of wound colonization in severely burned
patients: a retrospective analysis. Bums, 18: 98-102,1992.
- Van der Waay D., Manson W.L., Arends J.A. et al.: Clinical
use of selective intestinal decontamination: the concept. Intensive Care Med., 16: 5212,
1990.
- McMillan B.G., Holder I.A., Alexander J.V.: Infections in
burn wounds. In: "Hospital infections", Bennet J.V., Brachman P.S. (Eds), Little
Brown, Boston, 1986.
- Herruzo-Cabrera R., Garcfa-Torres V.; Rey-Calero J.,
Vizcaino-Alcaide M.J.: Evaluation of the penetration, strength, bactericidal efficacy and
spectrum of action of several antimicrobial creams against isolated microorganisms in a
burn center. Bums, 18: 39-44, 1992.
- Rotman K.J.: "Epidemiologia Moderna". Dfaz de
Santos,Madrid, 1987.
- Kleinbaurn D.G., Kupper L.L., Morgenstern H.:
"Epidemiologic Research", Van Nostram Reinhold, New York, 1983.
- Inoue S., Peck M.D., Alexander W.: Fungal translocation is
associated with increased mortality after thermal injury in guinea pigs. J. Bum Care
Rehabil, 12: 19-22, 1991.
|