| Ann. Medit. Burns Club - vol. 6 - n. 3 - September 1993
THE BURNED HAND: ITS CONSEQUENCES FOR THE PATIENTS'
PSYCHOLOGICAL STATUS AND SOCIAL READJUSTMENT
Striglis C., Tsutsos D., Panayotou R, Papagelis M.,
loannovich J.
Centre of Plastic Surgery and Microsurgery, General State
Hospital of Athens, Greece
SUMMARY. This study considers
the psychological effects of burns to the hands. It is based on the results of the
treatment of 74 patients with hand burns, seen over a 2-year period. A number of
parameters of social readjustment were considered, including work productivity and
self-care ability. It was found that long periods of hospitalization were related to the
subsequent development of a psychological disorder. Surgeons must consider not only the
aspect of correct initial treatment but also that of long-term consequences.
The burned hand has always been a
challenging problem for the surgeon, not only because of its surgical difficulties but
also because of the postoperative consequences for the patients' psychological status and
social readjustment. These consequences are often severe and more troublesome to patients
and surgeons than the initial injury itself. The purpose of this study is to consider the
effects the burned hand has on the patients' personality and social life. Seventy-four
patients with burned hands, out of a total of 228 burn patients, were treated in the Burns
Centre of the Athens General Hospital during the period 1990-91.
The age and sex of the patients is shown in Fig. 1. The distribution of patients with
burned hands is very similar to that of patients with bums of other anatomical sites.
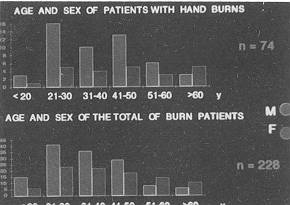 |
Fig. 1 |
|
Treatment of the burned hands was a) surgical,
using skin grafts and flaps, or performing an amputation; and b) conservative.
Evidently the cause of the bum is important in the decision as to treatment. The
majority of thermal bums (38) were treated surgically and the rest (22) conservatively.
Electrical burns very rarely require conservative treatment exclusively, whereas chemical
bums are usually treated conservatively.
A questionnaire was given to our patients after a follow-up period of six months to one
year in our Outpatients Department. The questionnaire focused mainly on the consequences
that burned hands had for the patient's psychological status and social readjustment. The
post-bum physical condition of the hand was classified according to the degree of scarring
on the patients'hands.
Patients with no post-bum sequelae on their hands were classified as "no
scarring" (11 patients). Patients with some mild sequelae but no restriction of their
hands' R.O.M. (range of movement) were classified as "moderate scarring" (31
patients).
Patients with contractures were classified according to the restrictions caused to R.O.M.
in two categories: the first contracture category with reduced R.O.M. (27 patients) and
the second with significantly diminished R.O.M. due to severe contractures (5 patients).
Social readjustment was evaluated using the following parameters:
Return to work period
a) Patients with no scarring returned to work after 52
days, on average.
b) Patients with moderate scarring returned to work after 157 days, on average.
c) Patients with contractures (reduced R.O.M.) returned to work after 199 days, on
average.
d) Patients with severe contractures (significantly diminished R.O.M.) returned to work
after 360 days, on average.
Productivity at work
a) All patients with no scarring had full work
productivity.
b) 83.8% of patients with moderate scarring had full productivity, 9.6% had reduced
productivity and 6.6% had limited roductivity.
c) 26.3% of patients with contractures had full productivity, 57.9% had reduced
productivity and 15.8% had diminished productivity. (Fig. 2)
d) 100% of patients with severe contractures had limited work productivity.
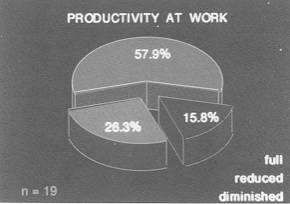 |
Fig. 2 |
|
Post-hospitalization employment status
a) All patients with no scarring had full post
hospitalization employment status.
b) 83.8% of patients with moderate scarring were employed. 9.6% were partially employed
and 6.6% were unemployed.
c) 25.9% of patients with contractures had full employment, 48.2% were partially employed
and 25.9% were unemployed. (Fig. 3).
d) 60% of patients with severe contractures were on a pension and 40% were unemployed.
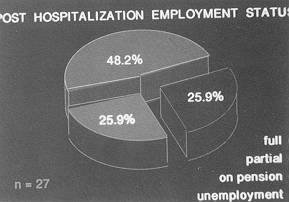 |
Fig. 3 |
|
The consequences jorfamily life and leisure time
a) Patients with no scarring suffered no consequences
in their family life and leisure time.
b) 96% of patients with moderate scarring suffered no consequences in their family life
and leisure time, and 4% some consequences in their family life.
c) 74% of patients with contractures suffered no consequences in their family life, 22%
suffered some consequences, and 4% suffered serious consequences.
d) 40% of patients with severe contractures suffered moderate consequences and 60%
suffered serious consequences.
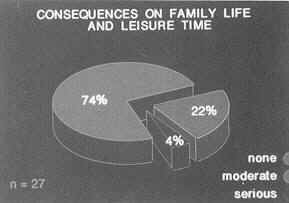 |
Fig. 4 |
|
Self-care ability was also evaluated as a
parameter of social readjustment
a) Patients with no scarring had full self-care ability.
b) Patients with moderate scarring also had full self care ability.
c) Patients with contractures had 81.5% full and 18.5% partial self-care ability.
d) Patients with severe contractures had 20% full, 40% partial and 40% reduced self-care
ability. (Fig. 5)
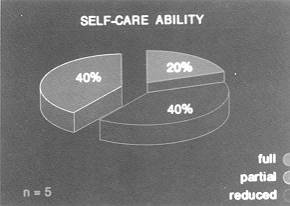 |
Fig. 5 |
|
The psychological status of the patients,
i.e. whether they were psychologically healthy, had a pre-existing disorder or developed a
post-burn psychological disorder, was evaluated using the following parameters:
a) Appointment with a psychiatrist.
b) Use of relevant medication.
c) Need for in-patient psychiatric treatment.
Results revealed that the longer the
hospitalization period the higher the incidence of the development of a psychological
disorder. (Fig. 6)
In conclusion, patients with burned hands suffered serious consequences as regards their
psychological status and social life. These consequences were related to the degree of
post-burn sequelae and the physical condition of the hands. The surgeon should always bear
in mind how important the hand is for the burn victim's social readjustment and mental
status, and he must not only aim at correct and early initial treatment but also consider
the equally important follow-up and guidance after the patient's discharge from hospital.
Only in this way will the burn patient manage to readjust to social life and overcome the
psychological impact of the burn disease.
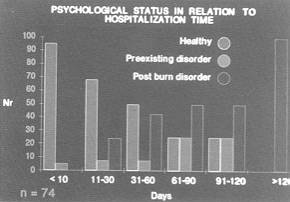 |
Fig. 6 |
|
RESUME. Cette étude,
qui prend en considération les effets psychologiques des brûlures aux mains, est basée
sur les résultats du traitement de 74 patients atteints de ce type de brûlure suivis
pendant une période de 2 ans. Nous avons considéré divers paramètres de la
réadaptation sociale, y compris la productivité de travail et la capacité de se soigner
soi-même. Nous avons constaté que les longues périodes d'hospitalisation étaient
associées au développement successif de troubles psychologiques. Les chirurgiens doivent
donc considérer non seulement l'aspect du traitement initial correct mais aussi celui des
conséquences à long terme.
|