| Ann. Medit. Burns Club - vol. 6 - n. 4 - December 1993
HYPERCOAGULATION IN BURN PATIENTS
- EFFICACY OF THROMBOEMBOLIC PROPHYLAXIS
Arevalo Velasco A., Del Campo Balsa
T, Gomez Bajo G.,* Cuesta Garcia V., Garcia Muhoz S., Lopez Pastor A., Fernandez-Chacon
J.L., Fernandez-Pavon A., Garcia Torres V.*
Analytic Haemotology Department, La
Paz Hospital, Madrid, Spain
* Burn Unit
SUMMARY. Sixty-nine
patients admitted to our hospital with bums, most commonly deep-dermal, of different
extent and production mechanism were studied. Heparin prophylaxis was administered to all
these patients, 18% with non-fractionated heparin (one dose every 12 hours) and 82% with
low molecular weight heparin (Tedelparine-BoxoF). A coagulation study was performed on
admission and 5, 10 and 30 days later. The results obtained support the existence of a
state of hypercoagulation, due mainly to a decrease of antithrombin III to thrombogenic
limits which tends to become normal as it evolves. We consider that this prophylaxis,
administered even in the absence of thromboembolic disease, is positive.
Introduction
Thromboembolic venous disease
(TVD) is today one of the most important causes of morbidity and mortality. Pathology
related to burn injuries is outstanding among TV13 risk factors in non-surgical patients.
The incidence of pulmonary embolism, the most severe complication of TVD, ranges from 5%
to 7% in bum patients (1). The activation of haemostatic factors, the appearance of
disseminated intravascular coagulation (DIC) and long stays in bed have been considered
pathogenic factors of this complication (2). In a previous study (3), we described the
decrease of antithrombin Ill (AT 111), the most important inhibitor of thrombin
production, in this pathology. This decrease is considered to be one of the basic
aetiologies of the thrombotic phenomenon; for this reason, considering the certainty of
the risk, we propose in this pathology prophylactic therapy with subcutaneous heparin. The
objectives of this study were thus to evaluate the efficiency of heparin prophylaxis, to
analyse the behaviour of AT Ill and to study how basic coagulation parameters evolve with
this treatment.
Material and methods
Sixty-nine patients admitted to
the Bum Unit of our hospital, mostly with deep-dermal burns (age range 10 to 92 yr,
average: 43 ± 21 yr; 19 females and 50 males) were studied.
Burn wound extent ranged from I to 90% (average: 34.5 ± 22.8%). 52.8% of the patients had
a TBSA between I and 30%, 34.7% between 31 and 60% and 12.5% over 60%. Regarding the burn
mechanism, in 59 cases the lesions were produced by flame, in three by scalds and six by
electricity.
Prophylaxis with subcutaneous heparin was administered to all the patients:
non-fractionated calcium heparin (NFH) every 12 h to 18% and low molecular weight heparin
(LMWH) (TedelparineBoxol', at high-risk dose: 5000 Ul) every 24 hours to the other 82%.
This prophylaxis was administered from admission until the risk had disappeared.
The study was performed on admission and 5, 10 and 30 days later.
Blood samples were obtained by venous puncture and distributed in various tubes: one with
EDTA for platelet count, another with fibrinolysis inhibitors to determine serum
fibrinogen degradation products (FDP), and two others with sodium citrate in a proportion
of one to nine for the other parameters.
The following measures were made: platelet count (in a HI device, Technicon); prothrombin
activity, APTT and fibrinogen, according to Caen et al., with an automatic technique
(Electra 900, MLA); FDP with the latex technique; and AT III using a chromogenic substrate
method in ACL 300.
The statistical analysis was performed using linear regressions, analysis of variance
(ANOVA) and Student's t test.
Sixteen patients died during the study: one of DIC, one of a haemorrhagic disease and the
other fourteen of non-haematological causes. All the other patients recovered.
Results
The clinical evolution, as already
said, was good in 53 patients (76.81%), with 16 deaths (23.18%). Analysis of the causes of
death shows (Fig. 1) only two cases related to the coagulation system, one patient dying
of DIC and the other after a haemorrhage. Both patients were young, with deepdermal 80%
TI1SA bums. The blood disease appeared after admission and did not respond to substitutive
therapy. The rapid evolution prevented the use of thromboembolic prophylaxis and for this
reason the clinical pictures cannot be related to this therapy. A haemostatic study was
performed on the admission of the two patients but the mortal evolution prevented further
studies. The death of these patients supports the thesis of the importance of coagulation
abnormalities in critically injured bum patients, and underlines the necessity of their
control and treatment.
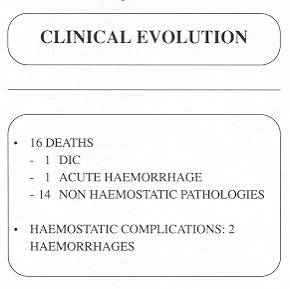 |
Fig. 1 |
|
The evolutionary results of the
haemostatic parameters are show in Table 1. Prothrombin time (PT) and APTT did not change
significantly in time. PT levels were normal after the first test, with a slight
nonsignificant decrease on day 10. Considering the results obtained with APTT, a
shortening was observed after admission and throughout the month of study.
The blood platelet (PIT) count was normal, showing a slight decrease with a subsequent
increase. These variations were significant but always remained within normal values,
except for the increase on day 10.
The fibrinogen plasmatic levels significantly increased from normal values after the first
test. These levels decreased gradually until day 30, but were still above normal values at
that time.
The FDP level showed a slight significant increase above normal values between the first
test and day 30. This increase, as we explain in the Discussion, reflects the tendency
towards hypercoagulation in these patients; this datum also suggests the presence of DIC.
The testing of AT 111 was intended to show whether this coagulation inhibitor plays an
important role in the thrombotic tendency observed in bum patients and how it evolves.
Considering all the patients, we found (Table I) a significant decrease in the AT 111
level at the first measurement. This level, which appeared in 70% of the cases, is an
important risk factor in thrombosis. When AT 111 levels range from 70 to 80% the
thrombotic risk is important, and when they go from 60 to 70% it is alarming. From day 5
onwards, AT 111 levels became normal in all patients. These data are shown in Fig. 2. In
many patients (66%) this level is below 80%, and more importantly 36% have levels below
60%. We can also see that AT III slowly became nomial after day 5 in all patients but
four.
Relating AT 111 levels to T13SA (especially when this area is >50%) we can notice in
the first test an inverse relation between AT 111 levels and T13SA.
Discussion
We noticed in our study an initial
increase in platelets and fibrinogen followed by a decrease. The behaviour of these two
parameters is compatible with their expression as acute phase reactants. The findings in
the literature are similar, considering the different chronology employed (4, 5).
An activation of the coagulation cascade also occurs at the same time. This is measured by
a shortening of APTT. This activation continued throughout the 30 days. This is an
important consideration to justify the administration of thromboembolic prophylaxis for a
long period. This prophylaxis must be administered, in our opinion, until patients achieve
two aims: active mobilization and the tendency of APTT to become normal. We consider this
non-specific test so important because clinical experience (6) shows that the prevention
of post-surgical deep venous thrombosis, in high-risk pathologies such as hip surgery, is
not achieved until the shortening of APTT is corrected through adjusted doses of heparin.
The standardized administration of this prophylaxis was effective in our study.
Prothrombin activity was kept within normal range after admission, which supports the
existence of a previously normal hepatic function.
There was no significant increase in FDR This fact, together with the increase in the
platelet count and fibrinogen, supports the absence of consumptive coagulation (DIC) in
our group, apart from the patient who died of DIC in the first hours of its evolution.
The initial decrease of AT III down to thrombogenic limits became normal as it evolved. If
the hepatic function is normal, we can assume that the decrease is due to consumption. The
inverse relation between AT III levels and TBSA has been discussed in a previous work (3).
Some studies try to relate AT III decrease in burn patients to alterations in granulocyte
enzymes (4-7). Heparin prophylaxis was administered in view of the thrombogenic risk in
these critically injured patients. In the first phase prophylaxis was performed with NFH
(8, 9) twice daily, because at this dosage it causes fewer haernorrhagic complications but
has the same antithrombotic efficacy (10). Some authors prefer to select patients in order
to avoid secondary effects, especially haemorrhage (1-11). Our experience supports the
principle of not excluding critically injured burn patients from this group of
prophylaxis, as they have an important thrombogenic risk and do not suffer haemorrhagic
complications when given this dose of NF14 (10).
We performed this study when low molecular weight heparins (LMWH) were beginning to be
used as prophylaxis (12, 13), and for this reason we used one of these products
(Tedelparine-Boxol') in almost all our patients. L~ owe their prophylactic use to their
condition as a main inhibitor of factor X. and to their better bioavailability, which
explains why they are an ideal antithrombotic agent. Clinical results in the literature
(14, 15) show a similar level of protection to NFH with a subcutaneous single dose every
day. This is an advantage that helps patients to manage long-time medication.
The evaluation of thrombotic incidence in our patients was clinical, as it was not
possible to perform methods for detection of deep venous thrombosis, owing to the great
extent of the burns.
The absence of thrombotic phenomena and haemorrhagic complications convinces us that this
prophylaxis administered to critically injured burn patients is positive.
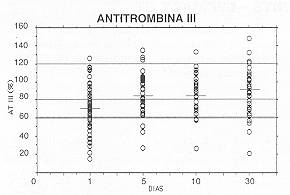 |
Fig. 2 |
|
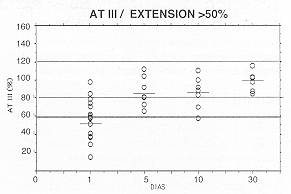 |
Fig. 3 |
|
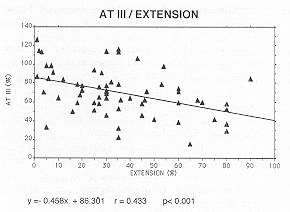 |
Fig. 4 |
|
RESUME. Les auteurs
présentent les résultats d'une étude sur 69 patients hospitalisés dans leur centre
atteints de brûlures, pour la plupart dermique-profondes, d'étendue et étiologie
diverses. La prophylaxie avec l'héparine a été administrée à tous les patients, 18%
avec l'héparine non fractionnée (une dose toutes les 12 heures) et 82% avec des
héparines de poids moléculaire bas (Tedelparine-Boxoll). Une étude de la coagulation a
été effectuée au moment de l'hospitalisation et après 5, 10 et 30 jours. Les
résultats de la recherche confirment l'existence d'une condition d'hypercoagulation due
principalement à la diminution de l'antithrombine III aux niveaux thrombogènes qui tend
vers la normalité comme elle évolue. Nous considérons que cette prophylaxie,
adininistrée même en absence d'une pathologie thromboembolique, est positive.
BIBLIOGRAPHY
- Purdue G.F., Hunt LL.: Pulmonary emboli in
burned patients. J. Trauma, 28: 218-20, 1988.
- Gehrke C.F., Penner J.A., Niederhuber J. et al.:
Coagulation defects in burned patients. Surg. Gynecol. Obstet., 133: 613-6,1971.
- Femàndez Pavôn A., Garcfa Torres V.: Alteracioncs
de la coagulaciôn en pacientes quemados. Cirugfa Plàstica Iber. Lat. Am., 10: 117-26,
1985.
- Davis J.M., Dineen P., Gallin J.L: Neutrophil
degranulation and abnormal chernotaxis after thennal injury. J. Immunol., 124: 1467-71,
1980.
- Cullen JJ., Murray D.J., Kealy G.P.: Changes in
coagulation factors in patients with burns during acute blood loss. J. Bum Care Rehab.,
10: 517-22, 1989.
- Leyvraz P.F., Richard J., Bachmann F., Melle G.V.,
Treyvaud J.M., Livio J.J., Candardjis G.: Adjusted versus fixed-dose subcutaneous heparin
in the prevention of deepvein thrombosis after total hip replacement. N. Engl. J. Med.,
309: 954-8, 1983.
- Prager M.D., Herring M., Germany B. et al.: Elastase
and al-protease inhibitor in bum wound exudates, J. Burn Care Rehabil., 12: 300-5,1991.
- Saliba M.J., Dempsey W.C., Kruggel J.L.: Large bums
in humans: treatment with heparin. JAMA, 225: 261-9, 1973.
- Berkessy S.: High dosage heparin treatment of large
bums. JAMA, 226: 1464,1973.
- Kakkar V.V., Corrigan T., Spindler J. et al.:
Efficacy of low doses of heparin in prevention of deep-vein thrombosis after major
surgery: a double-blind randomised trial. Lancet, 2: 101-6, 1972.
- Simon T.L., Curreri P.W., Harker L.A.: Kinetic
characterization of hemostasis in thermal injury. J. Lab. Clin. Med., 89: 702-11, 1977.
- Nurmohamed M.T., Rosendaal F.R., Buller H.R. et al.:
Low molecular weight heparin versus standard heparin in general and orthopaedic surgery: a
meta-analysis. Lancet, 340: 1526,1992.
- Hirsh J., Levine M.N.: Low molecular weight heparin.
Blood, 79: 1-17, 1992.
- Rosendual F.R., Nurmohamed M.T., Buller H.R., Dekker
E., Vandenbroucke LP--- Briet E.: Low molecular weight heparin in the prophylaxis of
venous thrombosis: a metaanalysis. Thromb. Haemost., 65: 927, 1991.
- Samama M., Bernard P., Bormardot LP., Combe-Tarnzali
S., Lanson Y., Tissot E.: Low molecular weight heparin compared with unfractionated
heparin in prevention of postoperative thrombosis. Br. J. Surg., 75: 128, 1988.
|