| Ann. Medit. Burns Club - vol. VI - n. 4 - December 1993
TREATMENT OF SMALL DEEP DERMAL AND FULL-THICKNESS BURNS WITH
A HYDROCOLLOID DRESSING
Garcia Torres V., Gomez Bajo G., Herruzo Cabrera
R.
Burn Unit, Department of Plastic Surgery, La Paz
Hospital, Madrid, Spain
SUMMARY. A study was
undertaken to determine not only the effect of a hydrocolloid dressing on the healing of
small deep dermal and full-thickness wounds but also its relation to other factors such as
age, mechanism, localization and, especially, bacterial colonization/ infection.
Fifty-five patients were studied in relation to subjective sensations (pain, discomfort,
odour), epithelialization phenomena and relative rates, bacteriological surveillance by
semiquantitative cultures, and sequelae.
Introduction
There is an endless series of
synthetic and biosynthetic dressings which are continuously recommended for use in topical
treatment of burn wounds. Thorough knowledge of even a part of them would require
full-time work in their study and experimentation.
Among all these new dressings, we have used in our Burns Unit at La Paz Hospital a
semipermeable hydrocolloid dressing, which owed its absorbent properties to
carboxymethy1cellulose. Various studies (2) have reported an improvement in healing rates
when using this kind of dressing compared to classical techniques. Its effect seems to be
due to its occlusive properties, as it creates a special microclimate that reduces healing
time, with better cosmetic results and less discomfort and pain sensation (1, 2, 3).
Material and Methods
Sheets of this dressing consist
(2) of a semipermeable polyurethane film coated with a flexible elastic mass (made from a
styrene-isopropene block copolymer together with polycyclopentadiene dioctyladipate) and
containing 42% sodium carboxymethylcellulose (NaCMC) as the principal absorbent (Figs
1-9). The application of these sheets was performed under aseptic conditions after washing
the wound carefully and covering the area to be treated with a gauze impregnated in
clorhexidine digluconate for five minutes. The frequency of change ranges from 2 to 4
days, with an average of 3.5 days. The mean number of applications was 4.41 (from 2 to 10)
(Table 1).
| Table 1
Epidemiological data |
| |
|
|
|
AGE |
55.27 YEARS |
|
|
SEX |
MALES 16 MALES / 39 FEMALES |
|
|
TBSA |
3.17% (0.1 TO 10%) |
|
|
DEPTH |
SUPERFICIAL DERMAL 10 |
DEEP
DERMAL 38 |
FULL-MICKNESS
8 |
| |
|
|
|
| |
NO |
SLIGHT |
INTENSIVE |
PAIN |
41 |
14 |
0 |
DISCOMFORT |
36 |
15 |
4 |
ODOUR |
40 |
13 |
2 |
PIGMENTATION |
32 |
18 |
5 |
HYPERTROPHIC
SCARS |
53 |
2 |
0 |
COSMETIC
SEQUELAE |
35 |
19 |
1 |
JNCTIONAL
SEQUELAE |
47 |
7 |
1 |
| |
|
|
|
EPITHELIZATION
COMPLETED |
16.08 DAYS
(FROM 8 TO 30) |
|
|
|
|
Fifty-five consecutive patients with small-size burns
(range: 0.1 to 10% TBSA) treated at our Bum Unit (in-patients and out-patients) between
June 1992 and January 1993 were included in the study. For each patient age, sex, cause of
injury, total body surface area burned, depth of injury, localization, previous pathology,
size of area treated with the dressing, previous treatment and days post-bum when dressing
was first used wore recorded. Bacteriological surveillance was performed by wound
semiquantitative cultures (4) before and after each application of the sheets. Subjective
sensations of the patients were also recorded: pain, discomfort, odours. Patients were
followed up after discharge in order to determine shortand medium-term cosmetic and
functional results and scar quality.
Results
Wound healing was achieved in 50
patients. The other five patients needed autografts to cover their wounds. Three of the
patients who needed surgery were over 70 years old, four suffered from previous vascular
diseases and one suffered a high-voltage electrical injury in the foot causing a
full-thickness burn involving tendons and bone.
The dressing proved to be well accepted by the patients. Fourteen patients reported slight
pain (Table 1) after application; 36 felt no discomfort, which was severe in only four
patients; and 15 perceived slight bad odour (strong in two cases). Surprisingly,
discomfort and pain had no relation to positive wound cultures and only a slight
correlation to odour.
The average length of time before complete healing was 16.08 days (range: 8 to 30 days).
When previous wound cultures were negative, the epithelialization time was shorter (14.46
days) than when they were positive (18.94 days). When wound cultures were negative after
application of the sheets, healing was achieved earlier (15.04 days) than when they were
positive (17.00 days).
The analysis of epithelialization quality related to colonization/infection of the wounds
shows similar results. When previous cultures were negative, excellent results were
obtained in 71.85% of the patients, and when positive in 55.55%. When organisms were
isolated after application of the sheets, excellent results were obtained in 60.71% of the
patients, compared to 71.42% in whom no organism grew.
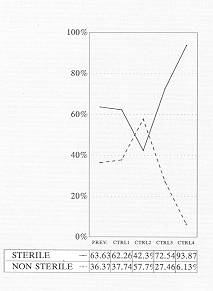
The microbiological data are shown in Tables H to VIII. Previous wound cultures were
sterile in 63.63% of cases. On day 8 after initiation of treatment with this hydrocolloid
(second control), micro-organisms were isolated in 57.70% of the cultures. At the fourth
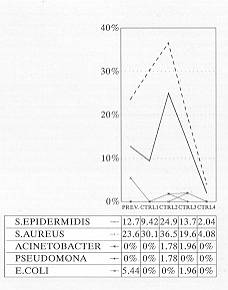
control (day 16), micro-organisms were isolated in only 6.13% of cases. The most frequent
micro-organisms were S. aureus (peak incidence (P1) 36.53%) and S. epidermidis (PI
24.98%). Gram-negative bacteria (E. Coli, Proteus, Pseudomonas) showed a very low
incidence.
Medium-term results (6 months) were predominantly good. Pigmented scars appeared in 23
patients (only five with very obvious pigmentation). We found no keloids in our patients
and only two of suffered from hypertrophic scars. Twenty patients developed cosmetic
sequelae which were severe in only one case; seven patients suffered slight functional
sequelae and one developed a serious problem, suffering mutilation of the foot after a
high-voltage electrical injury.
 |
 |
| Table II Bacteriological surveillance control
after second application |
Table III Bacteriological surveillance control
after second application |
 |
 |
| Table IV Bacteriological surveillance final
control |
Table V Bacteriological surveillance |
 |
 |
| Table VI Bacteriological surveillance positive
cultures |
Table VII Bacteriological surveillance positive
cultures |
|
Discussion
We have tried in this study to
assess the benefits of a hydrocolloid dressing after using it in our Burn Unit at La Paz
Hospital for a period of six months.
We believe that the best method for treating small deep den-nal and full-thickness burns
is early surgical debridement and immediate closure with autografts. Nevertheless, in
certain circumstances, with small-size burns, if surgery cannot be performed because of
previous pathology, anaesthetic contraindication or -not infrequently - because the
patient refuses any surgical procedure, we consider that this dressing is a good
alternative.
This dressing is mainly indicated for deep dermal burns and sometimes for full-thickness
bums. We have noticed that post-application pain, discomfort and bad odours are very
infrequent, which makes it better accepted by the patient than other topical therapies. We
have also noticed that epithelialization time is shorter than that necessary with
classical techniques, in agreement with previous reports (2).
What we have not seen in any previous study is a bacteriological surveillance of the
wound. These reports (5, 6) were based on clinical controls, which found no macroscopic
evidence of infection. When we tested the microbiological state of these wounds, by means
of seniiquantitative cultures, we found that in spite of the absence of antimicrobial
properties in this dressing infection was no more frequent than that expected when using
other antiseptic agents. Epithelialization was obviously achieved earlier when no wound
infection/colonization appeared. These results may be related to the improvement of
healing time.
To sum up, the careful use of this dressing under aseptic conditions offers a very good
alternative in the treatment of small-size deep dermal and full-thickness bums.
 |
 |
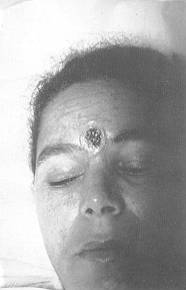
| Fig. 1 Self-inflicted
chemical bum in an attempt to remove a tattoo. |
Fig. 2 Surgical
removal of the eschar |
 |
 |
| Fig. 3 Application
of carboxyrnethylcellulose sheet. |
Fig. 4 Control
after 10 days of treatment. |
|
 |
Fig. 5
Final result |
|
 |
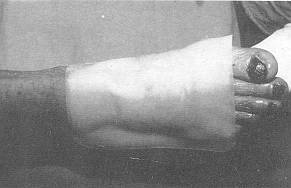 |
| Fig. 6 Contact
burn. Thirty days of evolution in other hospital. |
Fig. 7 Application
of carboxymethycellulose sheet |
 |
 |
| Fig. 8 Control
after fifth application |
Fig. 9 Final
result. |
|
RESUME. Cette étude
détermine non seulement l'effet d'un pansement hydrocolloïdal sur la guérison de
petites lésions dermiques profondes et à toute épaisseur mais aussi sa rélation à
d'autres facteurs comme l'âge, l'étiologie, la localisation et, particulièrement, la
colonisation/infection bactérienne. Les auteurs ont étudié 55 patients, en considérant
les sensations subjectives (douleur, malaise, odeurs), les phénomènes
d'épithélialisation, le contrôle bactériologique par les cultures sémiquantitatives,
et les sequelles.
|