| Ann. Medit. Burns Club - vol. VI - n. 4 - December 1993
THE CORRECTION OF THE INGUINAL-ABDOMINAL-GENITAL CONTRACTURE, WITH A CASE DESCRIPTION Belba GA Clinic of Plastic Surgery and Burns, U.C.H.T., Tirana, Albania SUMMARY. Through the description of a case with inguinal, abdominal and genital contracture, the author discusses the role and function of cutaneous triangles, emphasizing their importance when the pathology involves some entire regions.
Introduction In post-burn plastic surgery, the
role of angles and triangles and their transfer in the form of Zplasty is indisputable (1,
2, 7). Their creation in cutaneous folds gives the region the necessary mobility and
desired function. The realization of a triangle means applying economic incisions, using
autochthonous skin in a vascularised form, and minimising the use of epidermo-dermic
transplants. Anamnesis and local status The patient Z.R, 22-years-old, was
burned as a result of fire when four years of age. After wrong local treatment she was
affected by a scar contracture which she and her~parents underestimated. She married at
the age of 21 and came to be examined by us, while pregnant. She was sent by an
obstetrician in order to be helped to have a normal birth. The foetus had a normal
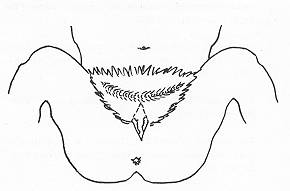
development of 21 weeks. 1 Locally the patient had a contracture in the fo of a web space
joining two inguinal regions in e centre, and impeding opening of the two infeior
extremities. In the upper part this had caused retraction of the abdominal region as far
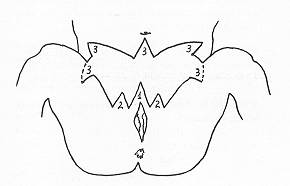
as the proximity of the umbilicus. Operative technique and case discussion By using a potentiated general and endotracheal anaesthesia with Fluothane, we managed to achieve full relaxation of the patient without damaging the foetus. With the patient in the gynaecological position the incision started on the pubis. We first created triangle number 1, size 5x3 em, which corresponded to the vertical orientation of the vulvar region.
Continuing alongside in both
directions, immediately out of the base of the first triangle we formed triangles number
2, size 3x2 em, which caused the elimination of the retractive forces and gave the
necessary mobility to the vulvar region, including the labia majora. The incisions then
passed in linear form into the two inguinal regions, finally creating angles number 3,
size 4x3 em. The purpose of these angles was to completely free the regions affected by
scarring and to frame them in relation with the femoral region, unaffected by scarring.
The same functions pertained to the other angles formed on the upper part of the operated
wound, also labelled number 3. This is the only possible way to realize an abdominal
opening sidelong and in the centre. We would emphasize that the sizes of the angles and
triangles should not be fixed. This depends on the extent of the scarring and the
stretching it causes to the tissues. The cutaneous defect, though covering a large surface
(25x20 em), was covered by epidermodermic transplant. The median and posterior part of the
right femoral region served as the donor site. Conclusion Most vicious post-burn contractures require covering of the wound with epidermo-dermic transplant. It is the plastic surgeon's job to plan proper incisions, to interrupt the retractive forces and to form a new line of forces without tension, in an attempt to approach the initial function. This can be realized through imaginative location of the angles and triangles, especially by combining their reciprocal actions. RESUME. L'auteur, à travers la description d'un cas de contracture inguinale, adbominale et génitale, discute le rôle et la fonction des triangles cutanés, en soulignant leur importance quand la pathologie intéresse des régions entières. BIBLIOGRAPHY
|