| Ann. Medit. Burns Club - voL VII - n. I - March 1994
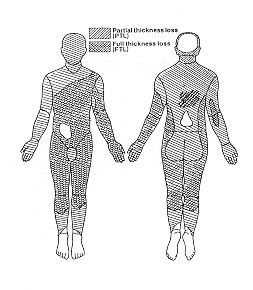
MANAGEMENT OF EXTENSIVE BURNS: A CASE REPORT Osman 0. F. Dr. Fakhry Hospital, Alkhobar, Saudi Arabia SUMMARY. An adult male patient aged 32 years sustained flame bums involving 95% of his body surface area (60% deep). Lactated Ringer's solution was used for resuscitation. Fresh plasma and whole blood were given early and repeated when indicated. Early enteral and parenteral nutritional support and systemic antibiotics were employed. Wound debridement was continued with hydrotherapy and topical silver sulphadiazine cream. Physiotherapy and active and passive splinting were offered. Amniotic membrane was used as a biological wound dressing. Autografting was completed in four successive surgical sessions. The patient was discharged for further rehabilitation, physiotherapy and surgical reconstruction at the end of four months' hospitalization. Introduction During the last 30 years the death rate from bum shock has declined dramatically. This improvement in early bum care is due to an improved under-standing of the pathophysiology of shock after bum injury and to the wide diffusion of this knowledge among health care professionals. The major concern in the management of bums is no longer simply the survival of the patient but also includes morbidity and long-term rehabilitation and reconstructive problems. In deep burns necrotic skin serves as an excellent culture medium for micro-organisms to proliferate, and invasive infection will inevitably ensue if the lesion is not promptly resurfaced. In the case of extensive deep burns, after removal of the bum wound eschar it is impossible to cover the exposed wound completely with autografts because of the scarcity of donor sites. A variety of biosynthetic and biological dressings can serve as a temporary wound closure with different degrees of acceptability (1, 2, 3). The correlation between burn severity and the magnitude of the impairment of host resistance is well documented (4, 5, 6, 7, 8). Early nutritional support of the extensively burned patient is very important to reduce the accompanying catabolism and to preserve organ functions during the successive hyperinetabolic state, and above all to counteract the effect of catabolism on the body's immunocompetent system of defence against invading micro-organisms (9, 10). An important goal in the course of treatment of the burn patient is to facilitate from the outset the patient's eventual reconstruction and rehabilitation, i.e. to return the patient to society as a functional human being who is as aesthetically acceptable as possible (11). Case presentation A male patient aged 32 years was admitted to our hospital 25 minutes after sustaining a flame burn injury involving about 95% 13SA (60% of it deep) (Fig. 1). After first-aid measures in the emergency room, the patient was kept under intensive care with monitoring of his vital signs. Resuscitation started with lactated Ringer's solution at a rate of 3 mllkg body weight/percentage burn, and finally adjusted according to central venous pressure and urine output monitoring.
Shortly thereafter longitudinal escharotomies were indicated in the patient's chest, abdomen and left arm. There were no tracheopulmonary inhalation injuries. Antibiotics were started and continued according to wound flora monitoring. H, blocker (ranitidine) was started intravenously and continued orally. Serum electrolytes were finely adjusted at normal levels all the time. Fresh whole blood and plasma were started 24 hours after admission and continued as indicated. The limited number of available veins was mapped and continuously used.
Early oral intake was encouraged and proceeded to a high-protein high-calorie diet supplemented with the parenteral administration of Intralipid and an essential amino acid formula to reach the calculated daily calorie needs. Parenteral and subsequently oral polyvitamins, minerals and trace element formula were continued. Burn wound debridement with hydrotherapy was initiated and continued with wound flora monitoring. Antiseptic techniques were rigorously followed in dealing with the patient. Silver sulphadiazine 1% cream was used topically for the wounds with meticulous care of the urinary catheter and intravenous lines. Amniotic membranes were used as a biological dressing to cover superficial and deep wounds before and immediately after grafting. Active and passive splinting with physiotherapy for most body joints was continued as the general and local conditions permitted, and the patient's psychological condition was supported by all the attending personnel guided by our consultant psychiatrist. The patient's condition passed through periods of stability and instability with toxic manifestations, including diarrho~a and vomiting which were treated symptomatically. In the six weeks following admission surgical wound debridement under general anesthesia was performed in two sessions with continuous covering of the wounds with amniotic membranes. During this period healing of the superficial and deep dermal wounds was completed to reduce the raw areas to about 60% BSA. In this phase the deeply burned left hand showed necrosis of the fingers with exposure of the bones, joints and tendons, leading to amputation at the level of the metacarpophalangeal joints. Permanent wound closure with autografting was performed in four successive sessions at 10-15 day intervals using repeatedly the limited available healthy skin, including the scalp and some of the healed superficially burned skin. Locally, the wounds showed satisfactory graft take and complete healing of the donor sites, with a marked improvement in the patient's general condition and a gain in weight. In spite of the continuous physiotherapy and the active and passive splinting, the patient developed contractures, limitation of the full range of movement of some joints, and hypertrophic scars. He was discharged four months after admission for out-patient department follow-up with continuous physiotherapy and wearing pressure garments (Fig. 2). Later on, four consecutive reconstructive surgical operations were conducted to relase the contractures and to reconstruct the hypertrophic scars. In the meantime the rehabilitation department helped the patient to return to society as a functional individual. Discussion The burn is one of the most severe types of injuries the human body encounters. Its major consequences are not only mortality but also the tremendous morbidity and the cost factors that are involved. In extensive burns the health care personnel priorities at the time of injury are survival, functionality and cosmetics.In this case we were lucky to receive the patient immediately post-burn, without any other associated trauma, without pulmonary damage due to inhalation and without any pre-existing disease.As in most critical therapy, fluid resuscitation was tailored to the patient's, physiological responses and during the course of management we used total enteral with supporting peripheral parenteral nutrition, which includes the infusion of electrolyte-enriched isotonic solutions of amino acids, glucose and lipids, vitamins, oligoelements and insulin. According to the two-phase metabolic response to burning described by Cuthbertson and Tilstone (12), the major expenditures were on the third to fifth days after successful resuscitation.Our goal therefore was to determine the nutritional demands and to begin to deliver them as soon as the ileus was resolved. We satisfactorily used the Cufferi formula (13) which provides nutritional needs by giving 25 kcal/kg of body weight, plus 40 kcal/percent BSA burn, in glucose to nitrogen ratios of between 100:1 and 150:1. The patient's nutritional support was mainly enteral in order to reverse the immune defects (14, 15). By meticulous care of the urinary catheter and intravenous lines, urinary tract infection and suppurative thrombophlebitis never occurred throughout the period of treatment. In view of the known ability of the burn wound to contract, the patient was positioned to prevent contractures immediately on admission. This was supplemented with appropriately fashioned static and dynamic splints and with intensive physiotherapy (16).In this case burn wound debridement and complete excision of the eschar were not performed as early as they should have been because of many factors, some related to the patient, such as the extent and distribution of the deep bums, the scarcity of donor sites and the stability of his general and local conditions, and others related to limitations in the facilities available in our hospital.During each of the grafting sessions we only harvested the skin graft in the operating theatre, applying it a few hours later in the ward with simple bedside facilities. This shortened anaesthesia time, saved operating theatre time, decreased the chances of graft loss during post-operative transportation and recovery, and allowed minimal interruption of the patient's enteral nutritional regimen.According to the mortality probability charts (17, 18) and the prognostic burn indices (19, 20, 21, 22) this case should have had limited chances of survival, but with the determined hard work of the management team we succeeded in obtaining a good result.
RESUME. Un patient adulte mâle de 32 ans a subi des brûlures par feu qui ont intéressé 95% de la superficie corporelle (dont 60% profonde). Pour la réanimation nous avons employé la solution de lactate de Ringer. Le plasma frais et le sang entier ont été administrés précocement, et répétés selon les indications. Le patient a reçu le support nutritionnel entéral et parentéral précoce et les antibiotiques systémiques. Le débridement de la lésion a été continué avec l'hydrothérapie et la crème de sulfadiazine argentique appliquée topiquement. Nous avons employé aussi la physiothérapie et les attelles actives et passives. Comme pansement biologique pour la lésion nous nous sommes servis de la membrane amniotique. Le processus de l'autogreffe a été complété en quatre séances chirurgicales successives. Après quatre mois d'hospitalisation le patient a été renvoyé pour continuer la réadaptation, la physiothérapie et la reconstruction chirurgicale. BIBLIOGRAPHY
|
||||||||