| Ann. Medit Burns Club - voL VII - n. I - March 1994
THE USE OF TISSUE EXPANSION IN BURNS SEQUELAE Pérez Barrero P., Duato F., Agullô A., Gonzàles Labasa M., Vistôs J.L., Cimorra G.A. Plastic and Reconstructive Surgery Department and Regional Burns Unit, Hospital Miguel Servet, Zaragoza, Spain SUMMARY. Tissue expansion has become a very useful tool in the reconstruction of aesthetic and functional burns sequelae. In this paper we review a series of 56 expansions in 44 patients with burns sequelae treated in our department. We describe the technique and complications. According to our experience, the use of soft-tissue expansion for the reconstruction of scarred deformities in burn patients has proved to be a technique with optimal aesthetic and functional results. We therefore believe that controlled tissue expansion should be considered an extremely useful technique in the burn patient and should he selected when considered as an alternative. Controlled tissue expansion is a very worthwhile tool for the plastic surgeon who approaches the reconstruction of burns sequelae by covering the defects with adjacent donor tissues of similar colour, innervation, hair-bearing qualities and texture, leaving intact the adjacent skin structures. This technique has the unique characteristic of providing us with extra tissue without leaving an unsightly donor site.The sequelae of most burn wounds involve a certain degree of contracture, even if wound healing is by epithclialization of a graft. To have a shortage of donor tissue with similar characteristics is almost the rule. Furthermore, when we are planning the correction of the resulting deformities we should consider that the real defect is usually greater than the apparent one.The increase in vascularity produced during the expansion enables us to produce larger, reliable and predictable flaps. It also makes it easier to close donor sites.This technique therefore offers new prospects for treating burns sequelae because it allows us to increase the amount of surrounding non-affected skin and to use it to cover the excision of scarring wounds by local or distant flaps.In the light of present-day experience, the technique is now available to all plastic reconstruction surgeons. Like any other technique tissue expansion has some disadvantages, including the necessity of two - or even more - surgical procedures as well as multiple visits to the out-patients clinic. There is also a certain discomfort while expansion is taking place, plus a transitory cosmetic defect as the expanders become larger and therefore highly visible. Material and methods All patients with tissue expanders
placed between 1988 and 1992 in our Service were reviewed. In this 5-year period, we
placed 56 expanders in 44 patients who had suffered burns sequelae.
Two expanders were used simultaneously in
nine patients (5 in the scalp, 2 in the face, 2 in the lower limbs). In another patient we
used four expanders in the trunk. Surgical technique Pre-operative counselling with the
patients is essential. They must be aware that cosmetic deformities will occur during
expansion; that at least two surgical procedures will be required; and that they could
suffer mild discomfort during expansion. An informed and well-motivated patient will
tolerate this much better. First stage The patient is subjected to general
endotracheal anaesthesia, through a conveniently placed incision, and a subcutaneous
pocket is dissected (subgaleal in the scalp). The size of the pocket must be sufficient to
accommodate the temporary implant, which must remain with a smooth surface filling it
adequately.
Implant inflation We begin expansion two to four weeks after the incision of the implant placement has healed. For successive inflations we use saline with the addition of a certain quantity of dye (Bonney's blue) to facilitate location of the filling port. The amount of fluid injected each time is not subject to any rule: it is individualized according to the degree of tension and blanching of the skin, and to patient comfort. The filling sessions are usually at one-week intervals. In our series the expansion time ranged according to the region (Table II).
Second stage When the planned expansion has been completely achieved, the patient is re-admitted one day before the next surgical procedure. With the patient under general anaesthesia the expander is removed, the flap redesigned and the defect excised in accordance with the available tissue. This sequence is important in order to avoid creating an excised defect and a flap with insufficient skin to cover it. We do not make capsulotomies, in order to avoid damage to the neovascular net which grows around the capsule.
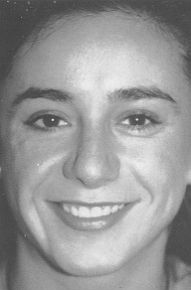
One-layer closure is suitable for the scalp. In other regions the suturing is performed in two layers. In this second phase we do not use any solution containing adrenalin to reduce bleeding, since it has been proved experimentally that the addition of this substance, even in a proportion of 1 to 200,000, markedly decreases the survival of delayed flaps. Case 1 Girl, 17 years old, with 55-mm-diameter scar over the right cheek-bone where, three months earlier, she had suffered a deep contact burn which was debrided early and covered with mid-thickness Wolfe-Kraus grafts. We planned a rotation-advancement flap from the adjacent skin of the cheek, placing a 200 mI expander (Fig. ]A) under it in order to get sufficient cutis. We proceeded with the expansion and ten weeks later excised the scar and covered it with the expanded flap. There were no complications and the result was acceptable (Fig. ]B).
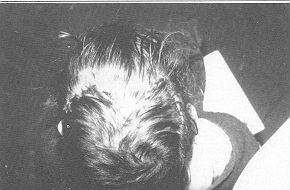
Case 2 Child, aged 5 years, showing post-burn alopecia 100 mm in diameter over the right parietal region due to an injury sustained two years before. We designed a rotation flap to cover the defect and expanded it with 150 ral placed subgaleally over the parieto-occipital region (Fig. 2A). After 9 weeks' expansion we removed the alopecia (Fig. 2B) and covered the area, advancing the expanded flap (Fig. 2C).
Case 3 Long-lasting scars over the anterior and inner face of both thighs in a 19-year-old girl who had suffered deep dermal burns 9 years previously (Fig. 3A). We used two expanders, 700 mI on the right leg (Fig. 3B) and 640 mI on the left. Nine weeks later we excised the scars and advanced the flaps covering the defects (Figs. 3C and 3D) without any post-operative complication.
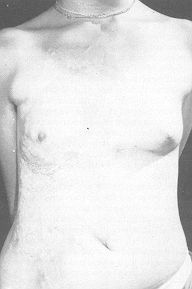
Case 4 Large post-burn scar on the trunk of a girl aged 15 years affected by thermal lesions when she was a child (Fig. 4A). Four large expanders were used, placed around the defect, and the period of inflation was 11 weeks (Fig. 4B). The result is shown in Fig. 4C. We are waiting for the girl to grow a little more before carrying out a right breast reconstruction procedure. Results Fifty-six expanders were used, with
complications in just 6 cases (10%). The complications were classified as major or minor.
The major complications were those that required removal of the expander or a change in
the initial planning. Three cases fell into this category (5%). Two of these (both in the
anterior cervical area) necessitated removal of the expander because of exteriorization.
In the third case (expander under the scalp), expander dislocation occurred, making
resettling necessary. In three cases (5%) minor complications were present: two patients
suffered a small suture dehiscence (one in the breast and one in the scalp); the third
patient, with a face expander, had a haematoma which was drained without further problems. Discussion When we are faced with the
reconstruction of postburn sequelae, we usually find a shortage of neighbouring donor
tissues with similar tissue properties. Furthermore, the real size of the actual defect
after excision of the scar is larger than that we see. This is due to the contraction
forces produced in every wound healed by second intention or with the use of thin
autologous skin grafts. RESUME. L'expansion
tissulaire s'est montrée une technique très utile dans la reconstruction des séquelles
esthétiques et fonctionnelles des brûlures. Cet article considère une série de 56
expansions chez 44 patients atteints de séquelles de brûlures traités dans notre
service. BIBLIOGRAPHY
|