| Ann. Medit. Burns Club - vol. VII - n. 2 - June 1994
ANTIMICROBIAL THERAPY PROBLEMS IN BURN SEPSIS Magliacani G, Stella M, Calcagni M. Dipartimento di Chirurgia Plastica e Centro Ustioni, Centro Traumatologico, Turin, Italy SUMMARY. This study concerns the difficulties of antimicrobial therapy, and analyses certain recently observed aspects in the treatment of sepsis, i.e. the utility of classifying bum patients in homogeneous classes, some particularities of pathogens, and effective methods for fighting them. The authors recommend use of Roi's Burn Severity Index, which makes it possible to classify patients in order to create comparable homogeneous groups. Regarding therapy, neither presumptive antibiotic therapy nor antibiotic prophylaxis seems useful, while single dose prophylaxis is indicated in some clinical situations. The authors recommend the use of vancomyein and teicoplanin against methicillin-resistant Staphylococcus, and of aminoglycosides, together with penicillin, against Pseudomonas aeruginosa. Introduction Evidence accumulated over several years of observation has shown that burn wounds are able to induce a series of effects resulting in severe alterations of the immune defence system, that burn patients are prone to infection, and that sepsis is the leading cause of mortality in the post-burn period. Some authors have, for this reason, suggested that infection is an unavoidable consequence in the clinical course of burn disease (1). In this paper we wish to analyse problems recently observed in the treatment of sepsis, in the light of our own experience and of the latest findings. We will review:
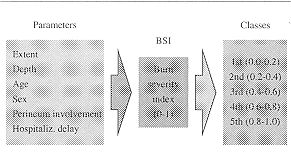
Risk indices Clinical observations show that the greater the extent of a burn the greater the gravity, and that the same burn has different prognoses depending on the patient's age (2). Consequently, if the variance of infection incidence is to be dependable it must be evaluated in patients having the same risk level. Of the various risk indices that have been proposed in an attempt to improve evaluation of the burn and therefore of its evolution (3), we have found the most interesting to be the Burn Severity Index proposed by Roi, which was based on a very large survey population (4). Although the presence of some important factors, such as associated tral nas and already existing pathologies, is not considered)i's Index provides a numerical value which enabled us to classify our patients in comparable homogeneous groups, which were distributed according to the numeric values given in the index (Tab. 1).
Our personal experience showed that classification of the patients in five groups was useful, as it was seen that infection was greater in its complexity (Tab. II), frequency (Tab. III), and as a cause of death (Tab. IV) as the risk class increased. The statistical significance of this diversified behaviour thus justifies the use of such an index to predict the infective destiny of the patient with a certain degree of accuracy and to evaluate the clinical and therapeutic protocol.
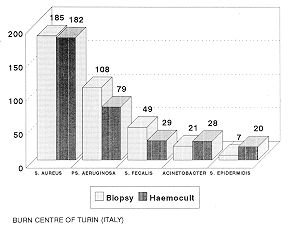
Particularities of pathogens We also observed that the aetiology of sepsis is correlated to the colonization of necrotic tissues by numerous pathogens, followed by multiplication with systemic invasion. This is confirmed by the fact that the micro-organisms were isolated in cutaneous biopsies and in haemocultures with almost identical frequency (Tab. V). There is considerable variability in the initial sepsis symptom complex and clinical diagnosis can be difficult, also because numerous factors complicate the diagnosis of infection in the burn patient (5). Wound infection diagnosis is important because it differentiates between wound colonization, wound infection and wound sepsis, which cause septicaemia. For this reason a reliable and accurate diagnostic procedure is a must: it is particularly important to make a differential diagnosis between sepsis and burn wound infection or burn wound contamination. The diagnosis therefore has to be based on complete microbiological cultures together with skin biopsies and serological tests. The result of the culture has to be examined very closely before any diagnosis of sepsis can be made, as the majority of pathogens responsible for sepsis behave as colonizers with similar frequency, and results obtained from superficial swab tests give limited diagnostic predictive results, whether negative or positive. Also, negative cultures very often underestimate sepsis (Tab. VI) and positive cultures may overestimate too high a percentage to be ignored (Tab. VII) (6).
Isolated bacterial flora has shown that in 92% of cases a mixed flora was present and the germs responsible are basically always the same: Staphylococcus aureus MR, Pseudomonas aeruginosa 8-lactamase producer, followed by Enterococcus, Proteus species, Escherichia coli, Candida Albicans and Acinetobacter Calcoaceticus anitratus, which frequently causes self-limiting epidemics. With reference to Staphylococcus aureus, we have to remember that besides its well-known resistance to methicillin there are newly acquired polyresistances that narrow the therapeutic choice down to vancomycin and teicoplanin. A new phenomenon is the passage of methicillin-resistance and later of polyresistance also to Staphylococcus coagulase negative, i.e. Staphylococcus epidermidis, with a remarkable increase in the frequency of isolation and in therapeutic difficulties (7). The main problem is the continuous occurrence of new resistances, and it is hazardous to propose to solve the problem while causes and modalities are still unknown. One reason for this failure would appear to lie in the illogicality of certain therapeutic practices. Many specialists believe that the use of antibiotics, or of some in particular, is the main determinant cause of antibiotic resistance. Opinion is going against the use of topical aminoglycosides. They enhance the production of enzymes such as transacetylase, adenyltransferase and phosphotransferase, which are known to be capable of inducing resistance. Also, some antibiotics are showing to be strong 6-lactamase inducers for certain bacteria, enhancing the creation of more aggressive strains. Cephalosporins have a greater responsibility than penicillins and with regard to Pseudomonas aeruginosa thienamycin-cilastatin seems to be the stongest inducer among all available drugs. Surprisingly, 6-lactamase inhibitors such as clavulanic acid and sulbactam have also shown an inducing activity for this enzyme. Therapeutic suggestions The strains responsible have often been found strongly resistant to tested antibiotics, making for a difficult therapeutic approach. Antibacterial therapy in burn patients is therefore a complex problem, with no easy solution, that cannot simply be overcome by the adoption of an appropriate antibiotic therapy or by the use of local antiseptics, which merely help to reduce the risk of skin lesion contamination. As yet, the rational use of immunological drugs in burn patients is restricted by the difficulty of correct assessment of the patients' immunological status and of precise identification of defective compartments, and by posttherapy checking of the return to normal values. Against methicillin-resistant Staphylococcus the use of vancomycin or teicoplanin is almost mandatory, but the percentage of eradication is low, especially in more severe cases (class 4 and 5). The difficulty of treatment encouraged us to undertake pharmacokinetic studies on vancomycin (8), in order to monitor antibiotic blood levels, to make any necessary posological adjustments in single doses and in the administration interval, and to reduce systemic toxicity (9). We are likewise proceeding with teicoplanin, and we are convinced that similar enquiries will be necessary for other molecules. As regards Pseudomonas aeruginosa B-1actainase producer, since aminoglycosides, alone or in association with other antibiotics, seem to have the best eradication rate, a chemotherapy with aminoglycosides together with penicillins may be suggested, avoiding monotherapy with thienamycin and cilastatin or quinolinol, because resistance strains are more and more diffuse. Presumptive therapy, i.e. any without culture result, should be avoided in routine activity. For the same reasons short- and long-term antibiotic prophylaxis is condemned to failure, because of the probable selection of increasingly resistant strains in the ward and in the patient. When rational therapy has not been established, some authors recommend single dose prophylaxis in the event of invasive procedures or contaminated surgical intervention, in order to minimize metastatic bacterial colonization (10). On this basis, we use teicoplanin (10 mg/kg) and a single dose (2 gm) of azthreonam. Conclusion A number of measures are necessary in the treatment of sepsis in burn patients, such as correct local care, nutritional support, environmental control and surgical therapy, all of which constitute an essential presupposition for effective treatment of infection. Early surgery, nutritional support and the use of suitable wards are of fundamental importance. They must be considered acquired knowledge and are therefore no longer a matter of discussion. There are however still some open problems in the field of antimicrobial therapy, and upon these we must focus all our efforts, in order to enhance patient survival. RESUME. Les auteurs, après avoir examiné les difficultés de la thérapie antimicrobienne, analysent certains aspe ets récemment observés dans le traitement de la sepsis, c'est-à-dire l'utilité de classifier les patients brûlés selon des classes homogènes, les particularités des pathogènes, et les méthodes les plus efficaces pour les combattre. Ils proposent l'emploi de l'Index de Sévérité des Brûlures de Roi, qui permet de classifier les patients pour créer des groupes homogènes. Pour ce qui concerne la thérapie il semble que ni la thérapie antibiotique prévue ni la prophylaxie antibiotique ne soit utile, même si la prophlylaxie à dose unique est indiquée en certaines conditions cliniques. Les auteurs conseillent l'emploi de vancornycine et de teicoplanine contre le Staphylococcus résistant à méticilline, et des aminoglycosides, conjointement avec la pénicilline, contre Pseudomonas aeruginosa. BIBLIOGRAPHY
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||