| Ann. Medit. Burns Club - vol. VII - n. 3 - September 1994
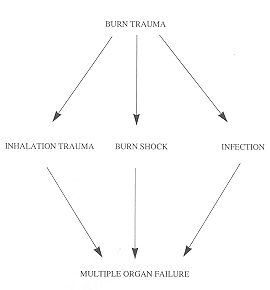
INDICATIONS FOR APPLICATIONS OF GLUCOCORTICOIDS IN BURN MEDICINE Hruba 1, Kénigova R, Drabek T. Burn Centre, Medical Faculty, Charles University, Prague, Czech Republic SUMMARY. This paper discusses various indications for glucocorticoids in bum medicine: first aid to burn victims, inhalation trauma, prevention and treatment of burn shock, and administration before initiation of antibiotic therapy when there is a threat of endotoxin shock. All these indications require short-term treatment with large doses of glucocorticoids. In the decision-making process regarding the adn-dnistration of glueocorticoids, it is necessary to consider the expected therapeutic contribution in relation to possible undesirable effects. The danger of multiple organ failure generally leads to the decision to give the patient glueocorticoids. An analysis is made of records of cases in which glucocorticoids were administered to bum patients in first aid. The causes of respiratory insufficiency in bum patients are also considered. The onset and development of bum shock, with release of vasoactive mediators, can be favourably influenced by glucocorticoids. When administered before bactericidal antibiotic therapy, glucocorticoids can prevent irreversible endotoxin shock. Burn trauma always creates tremendous stress in the affected person, evidence for which is provided by the elevenfold elevation in the catecholamine level. Immediately after the burn the patient is exposed to the risk of inhalation trauma and the development of burn shock, followed by localized or generalized infection. These conditions can lead to one of the major causes of death in burn patients: multiple organ failure (Fig. 1).
This paper deals with possible indications for glucocorticoid administration in burn medicine, namely:
All these indications require short-term
treatment with large doses of glucocorticoids.
The danger after this charge and of multiple organ failure usually leads to the decision to administer glucocorticoids to burn patients. We generally use 6alpha-methylprednisolone, which has the following advantages:
First aid First aid to a burned person is usually administered by mobile rescue workers. We analysed records of the administration by mobile rescue teams of glucocorticoids to 79 burn patients (adults with 20% or more burned body surface and children aged 3 years or over with 10% and more burned body surface). In the first hours post-burn glueocorticoids were given to 43 patients (54%) and not given to 36 patients (46%). Diagnosis of inhalation trauma was made in 33 patients, of whom 24 (73%) were given glucocorticoids. Inhalation trauma Inhalation trauma is caused by direct
thermal effect and by inhalation of the waste products of combustion. Burn shock Burn shock is the result of the failure of the regulation capacity of the affected organism. It develops relatively over a period of several hours, and is characterized by:
The fluid and protein loss leads to hypovolaemia,
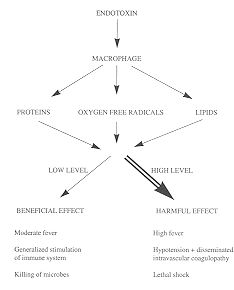
resulting in overproduction of catecholamines. Endotoxin shock When there is a risk of endotoxin shock, glucocorticoids are indicated before initiation of antibiotic therapy. Endotoxin is the lipolysaccharide of the outer membrane of gram-negative bacteria, and is released by their breakdown. It stimulates macrophages to produce three groups of mediators: proteins, lipids and oxygenfree radicals (5).
The tumour necrosis factor has a positive feedback and prostaglandin E2 a negative feedback for the synthesis of mediators. The effect of these mediators on the host organism is quantity-dependent (6). When the mediator level is low, their effects are favourable: mild fever, recruitment of microbe-specific and less specialized immune components, and microbe killing. When mediators are overproduced, their effects are harmful. They cause vasoparalysis, by the syndrome of leakage from the capillary bed, hypovolaemia, secondary hypoperfusion, disseminated blood clotting and consequently multiple organ failure (1, 7, 8, 11) (Fig. 2). The administration of bactericide antibiotics can cause the sudden disintegration of gram-negative bacteria. Previously administered 'glucocorticoids can alter lysis of the microbial wall and block the synthesis of mediators, preventing their overproduction and consequent harmful effects on the host organism. For these reasons we recommend the administration of glucocorticoids to burn patients 20 min before the first dose of wide-spectrum bactericide antibiotics in grainnegative infections. Conclusion The conclusion of this short communication is that in burn treatment large doses of glueocorticoids should be administered in rapid infusion at the appropriate moment. RESUME. Cet article considère les diverses indications pour les glucocorticoïdes dans le secteur de la médecine des brûlures: les premiers secours aux brûlés, le traumatisme d'inhalation, la prévention et la thérapie du choc de brûlure, et l'administration avant le commencement de la thérapie antibiotique en cas de risque de choc d'endotoxine. Toutes ces indications imposent le traitement de courte durée avec de grandes doses de glucocorticoïdes. Quand il faut décider sur l'administration des glucocorticoïdes, on doit considérer l'avantage thérapeutique prévu par rapport aux effets possibles non désirés. Le danger de l'insuffisance multiple organique conduit généralement à la décision d'administrer les glucocorticoïdes au patient. Les auteurs analysent des cas où les glucocorticoïdes ont été administrés aux brûlés pendant les premiers soins. En outre, ils considèrent les causes de l'insuffisance respiratoire. Le commencement et le développement du choc de brûlure, avec la libération des médiateurs vasoactifs, peuvent être influencés favorablement par les glucocorticoïdes. Les glucocortiedfdes administrés avant la thérapie antibiotique bactéricide peut prévenir le choc irréversible d'endotoxine. BIBLIOGRAPHY
|