| Ann. Medit. Burns Club - vol. VII - n. 4 - December 1994
A RETROSPECTIVE STUDY OF PATIENTS ADMITTED TO OUR BURNS UNIT Schembri K, Cacciottolo L, Swain C. St. Luke's Hospital, G'Mangia, Malta SUMMARY. Since the creation of a specialized burns unit in our hospital, 348 patients required treatment there during the five-year period 1989-1993. As all burned patients on the island of Malta are treated in this one facility, it is an ideal place to carry out epidemiological studies. Children, especially under five years of age, run the highest risk of burn injuries, Scalds in the patients' own home are the major cause of admission, Firework explosions are another significant cause. This retrospective study pinpoints areas that preventive programmes need to tackle and proposes ways as to how this may be done. Introduction The Burns Unit in St. Luke's Hospital,
Malta, has been functioning since 1989 (1). As it is the only burns centre on the island
of Malta, all patients requiring hospital treatment for burn injuries are admitted to it.
Patients with extensive bums or inhalation injuries are first admitted to the intensive
therapy unit.
In this study we have analysed patients requiring treatment for burn injuries. Emphasis is placed on those requiring in-patient treatment in the five-year period 1989-1993, The purpose of the study is to evaluate the age groups most commonly affected, as well as the commonest causes of to bum injuries. Method The statistical data for this study
were obtained from records of admissions to the Intensive Therapy Unit, and from patient
records kept at the Burns Unit. The latter include both personal data, from which the
patient's age on admission was obtained, and medical information. Results In the five-year period studied
(1989-93), a total of 348 patients required hospital admission for the treatment of burns.
The average hospital stay was 16 days. The annual intake was quite constant, namely 73,
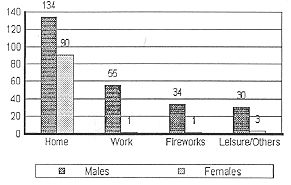
71, 64, 72 and 64 in the respective years. Of these, 253 (72.70%) were males and 95
(27.30%) were females. A total of 825 patients were seen on an out-patient basis. As the
population of Malta in 1991 was 359,543 (2), the incidence of bum injuries seen in
hospital was 0.02%.
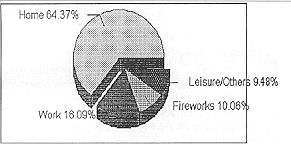
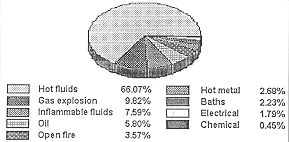
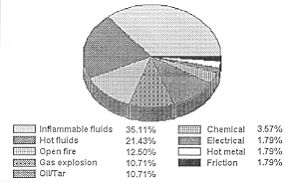
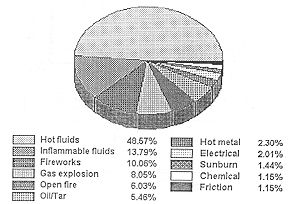
By far the commonest cause of admissions to the Burns Unit was scalding in the home. This accounted for 148 admissions, i.e. 66.07% of admissions due to domestic accidents and 42.53% of all admissions. Twenty-two admissions, i.e. 9.82% of admissions after domestic accidents, were due to the explosion of butane gas tanks, mainly used for powering gas ovens. Burns sustained at the place of work were most commonly caused by flammable fluids and hot fluids, such as steam.
A significant number of admissions (35,
equal to 10.06% of all admissions) were due to injuries resulting from the handling of
fireworks. Sadly, each year we still record a number of admissions following explosions in
firework factories or during village feasts. These accidents occasionally cause a number
of fatalities that do not reach hospital. A summary of all admissions according to their
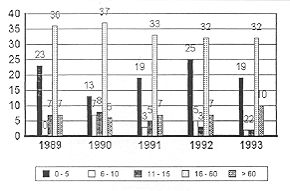
cause is given in Table III and Fig. 3. Discussion As in other studies (3, 5, 7, 8, 9), children under 15 years of age constituted a very large proportion of all admissions. The study shows a peak incidence in the 0-5 year age group, which constitutes more than one-quarter of all admissions. While other studies have reported the same finding (5,9), we point out that the incidence of burn injuries for this age group in Malta is very much higher than the average incidence for the whole population (see Table II). At this age, most children are looked after by their parents at home. However, this does not seem to prevent the occurrence of such accidents (10). Of note also is the fact that 48.85% of admissions were patients of working age (16-60 years). This represents a great socioeconomic burden owing to the total number of man-hours lost from work and the financial cost in terms of social benefits.
Scalds were the major overall cause of burns. This correlates well with other studies (3, 9, 11, 12, 13). Electrical and chemical burns were relatively minor causes. Another significant cause is related to misuse of fireworks.
The overall mortality rate is very favourable compared to other studies (3, 13). The low rate may be due to the relatively short distances in Malta and to the fact that nearly all the patients were treated from the first day postburn. Resuscitation was therefore immediately available. Conclusion Prevention programmes need to be set up immediately in order to reduce the risk of burn injuries, especially in the 0-5 year age group. Parents must be educated as to the risks involved at home, and especially in the kitchen. Such programmes should make parents aware of the dangers from the immediate post-partum period. Parents in Malta are already given a booklet concerning their child's health and well-being which also gives information about the birth and important milestone and vaccination schedules. We suggest that special warnings and a description of safety measures should be given to the parents with this booklet.
We would also like to see workers
and their employers more aware of the risk of burn injury. Protective clothing should be
made available and laws regarding its proper use enforced. Workers should not be required
to expose themselves to unnecessary risks.
Contacts with the health education authorities have been made regarding the implementation of preventive programmes. We also propose that a further similar study should be carried out after such programmes have been running for a significant length of time in order to assess the effect of the programmes on the number of admissions. RESUME. Les auteurs de cette étude rétrospective, depuis la création d'un centre spécialisé de brûlures dans leur hôpital, y ont traité 348 patients dans la période 1989-93. Puisque tous les patients brûlés dans l'île de Malte sont traités dans le même service, c'est un lieu idéal pour effectuer des études épidémiologiques. Les enfants, et en particulier les enfants âgés moins de cinq ans, sont les plus exposés au risque des brûlures. Lès ébouillantements dans la maison sont la cause principale de l'hospitalisation. Les feux d'artifice représentent une autre cause significative. Les auteurs définissent les zones que les programmes de prévention doivent attaquer et proposent les modalités pour les réaliser. BIBLIOGRAPHY.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||