| Ann. Medit. Burns Club - vol. V11 - n. 4 - December 1994
EPIDEMIOLOGY, CLINICAL TREATMENT AND THERAPY IN ELECTRICALLY
BURNED CHILDREN
Napoli B., D'Arpa N., Gullo S., Masellis M.
Divisione di Chirurgia Plastica. e Terapia delle
Ustioni, Ospeclale Civico e Benfratelli, USL 58, Palermo, Italy
SUMMARY. This research
reviews electrically burned children aged 0-12 years admitted to the Palermo Bums Centre
in the period 19751991. As regards the epidemiological aspects, apart from sex and age
distribution, particular attention is paid to the lesive agents and mechanisms responsible
for the burns and to the voltage of the electric current. From the clinical point of view
an account is given of the distribution of the burns according to the most frequently
involved sites (hand, mouth, forearm, wrist), followed by a discussion of the influence of
the localization of the lesion on the course of the disease and its treatment. The
distribution of patients is given on the basis of treatment (either exclusively medical or
medical and surgical). For the surgically treated cases the more significant procedures
for the functional recovery of the electrocuted upper limb are described.
In the period 1975-1991 we admitted to our
Burns Centre 132 children suffering from electrical burns. Boys (73.5%) outnumbered girls
(26.5%) with a male/female ratio of 2.7 to 1. The highest concentration of cases (82, i.e.
62.1 %) was in the 0-3 year age group (Table I).
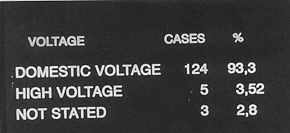
Burns caused by low voltage in the home environment were the most frequent (93.3%).
Play activities, such as the recovery of kites or birds' nests on power pylons, caused
some high-voltage bums in older children (3.5%) (Table II).
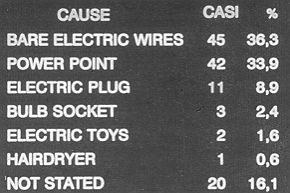
The list of causative agents, mainly exposed electric wires (36.3%), power points
(33.9%) and electric plugs (8.9%) - all in the home environment - indicates the lesive
mechanism of the electric arc by contact with these agents (Table III).
Contact generally occurs by direct handling: when electrified objects come into
contact with the mouth, the saliva, which is rich in electrolytes, completes the circuit,
transmitting the current through body tissues where resistance is lower.
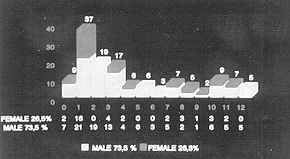 |
Table 1 -
Distribution by age and sex |
|
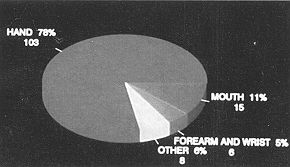
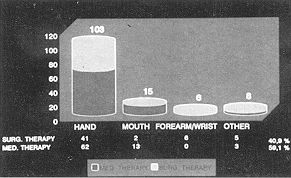
In 103 cases (78%) the lesion was in the
hands, in 15 cases (I I%) in the mouth, in six cases (5 %) in the forearm and wrist, and
in eight cases (6%) in other parts of the body (Table IV). Hand burns involved the
first and second fingers in 55 cases (53.4%).
The percentage of body surface area burned was very limited in all patients but two
(1.5%), in whom contact with high-voltage cables caused the ignition of clothing,
resulting not only in electrocution of the forearm and wrist but also an extensive fire
burn in 20% BSA in one case and 15% in the other. In all cases burns were third degree or
associated second and third degree.
Altogether 7 8 (59. 1 %) patients were cured with exclusively medical treatment, while 54
(40.9%) were treated surgically (Table V). Of the surgically treated patients,
forty (74.1%) were subjected to early surgery (within 20 days post-burn) while the other
fourteen (25.9%) had late surgical treatment.
As regards non-definitive surgical procedures (escharectorny, escharectomy and temporary
coverage with free skin graft) and multiple stage operations (flaps), the number of
operations performed was 78, equivalent to 1.4 per patient.
Case 1. G.G., age 1, girl
 |
 |
| Table II - Distribution
by current voltage |
Table III -
Distribution by causes |
 |
 |
| Table IV - Distribution
by site of lesion |
Table V -
Distribution by site and therapy |
|
 |
 |
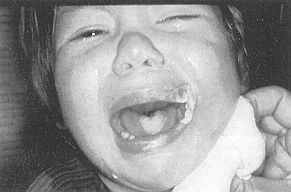
| Fig. la - Necrosis
due to electrocufion of tongue and left labial commissure. |
Fig. 1b - Lesion
in advanced state of cure after conservative treatment. |
|
 |
 |
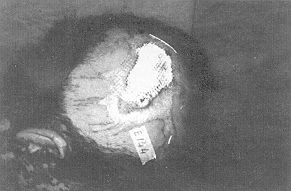
| Fig. 2a -
Necrosis due to electrocution of scalp. |
Fig. 2b -
Exposure, after escharectomy, of cranium; design of rotation flap performed on day 15. |
|
 |
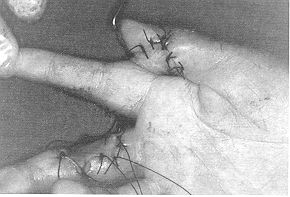 |
| Fig.3a -
Electrocution of first finger of left hand with exposure of long flexor tendon. |
Fig. 3b -
Cross-finger with second finger performed on day 22 |
 |
Fig. 3c -
Long-term functional recovery. |
|
 |
 |
| Fig. 4a -
Destruction of extensor apparatus and articular capsule of proximal interphalangeal
articulation of second finger of left hand recostructed with skin graft from ipsilateral
forearm. |
Fig. 4b -
Abdominal pouching on day 12. |
 |
Fig. 4c - Long-term
functional recovery. |
|
 |
 |
| Fig. 5a - Serious
electrocution of first and second finger of right hand with complete destruction of soft
tissues subjected to surgical debridernent on day 11. |
Fig. 5b - Coverage
with groin flap on day 16 after further debridement. |
 |
Fig. 5c - Functional
recovery. |
|
 |
 |
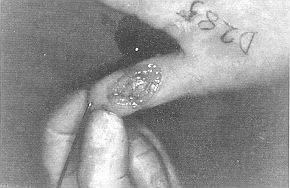
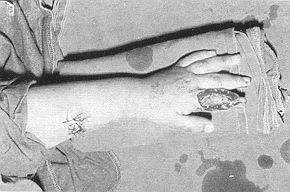
| Fig 6a -
High voltage double electric arch in right wrist |
Fig. 6b - Exposure
of ulnar vasculonervous bundle after escharectomy on day 15. Temporary coverage with skin
graft. |
 |
 |
| Fig. 6c - Exposure
of uIna after further escharectomy. |
Fig. 6d - After
reconstruction with abdominal flap performed on day 30. |
|
Discussion
The distribution by age and sex in our
patients is consistent with that found by other authors (1). This is also true of the
aetioPathogenetic aspects which - considering that we are dealing with children - may be
considered typical (contact in the home with objects in a state of low voltage).
Also typical, in relation to the aetiopathogenetic aspects, are the site and the
characteristics of the lesions, which are mainly in the hands and mouth and, although
localized and limited in extension, generally deep (1, 2, 3).
Most of the burns were treated and cured medically, since in addition to non-serious
lesions there are many others which due to their localization generally require
conservative treatment.
This is the case of mouth electrocutions, especially at commissure level, which can if
necessary be treated with secondary reconstructive procedures in the event of functional
sequelae (2, 4).
We never carried out any surgical procedures in the first post-trauma hours, as is on the
other hand recommended by some other authors (5, 6). However, compared to patients
operated late, more patients were subjected to surgery before day 20, when the lesion was
considered to be stable.
The definitive reconstructive techniques used are summarized in Table VL The
procedures followed were debridement, d6collement and juxtaposition of the edges, and
suturing in one case, and wedge excision and layered suturing in the other case, because
of haernorrhagic complications secondary to electrocution of the lower lip. In accordance
with the principle of greater simplicity we used dermoepidermal grafts whenever possible.
We used flap coverage when structures such as nerves, tendons, vessels, articulations or
bones were exposed. The demolition of nonviable segments of limbs was performed as soon as
possible in order to prevent possibly life-endangering complications (sepsis, kidney
failure) (6, 7,8)
Conclusion
The characteristics of the
distribution by age and according to aetiopathogenesis of the lesions show that the
prevention of electrical accidents in children is possible, and is based on:
- careful surveillance of younger children by adults;
- elimination of risk factors in the home environment;
- preventive education in older children and the population
as a whole (9).
Regarding the treatment of lesions caused by electric
current we would recall that:
- what may at first sight appear to be a serious and
extensive injury will in some cases heal with minimal sequelae;
- damage to the vessel intima may cause thrombosis even weeks
after the trauma.
A lesion due to electric current is thus a
lesion in evolution (4, 7); it is therefore of fundamental importance to make the right
choice between conservative and aggressive treatment and, if surgery is necessary, to
choose the right moment for reconstruction, i.e. either soon after the trauma or
subsequently, when the lesion has stabilized. We have seen that the site of the trauma may
determine the choice of the type of treatment; as to the choice of the right moment for
surgical procedures, our previous considerations would recommend a prudent and watchful
period of waiting. The reconstruction techniques are conditioned by clinical objectivity
and by the normal functions performed by the affected area; in children, reconstruction
using flaps involves an age-related risk factor due to their natural unawareness.and
restlessness.
SUMMARY. Les auteurs dans
cette étude considèrent les enfants atteints de brûlures électriques hospitalisés
dans le Centre des Brûlés de Palerme pendant la période 1975-1991. Pour ce qui concerne
les aspects épidémiologiques, ils ont analysé la distribution selon le sexe et l'âge
et en particulier les agents et les mécanismes qui ont causé les lésions et la tension
du courant électrique. Du point de vue clinique ils décrivent la distribution des
brûlures selon les zones corporelles les plus fréquemment atteintes (main, bouche,
avant-bras, pouls) et ils discutent l'influence de la localisation sur le cours de la
maladie et son traitement. Les données sont fournies relativement à la distribution sur
la base du traitement (soit exclusivement médical soit médical et chirurgical). Pour les
cas traités chirurgicallement les auteurs décrivent enfin les procédures plus
significatives pour la récupération fonctionelle du membre supérieur atteint de
brûlure électrique.
BIBLIOGRAPHY
- Rodrigues Menes H., Rigo Aguada A., Del Pino Paredes
V.: Epidentiologia, prevenci6n y tratarniento de las quemaduras electricas infantiles.
Cit. Plast. lber. Latinoamer., 14: 265-71, 1988.
- Kanzanjan, Converse: 11 trattamento chirurgico dei
traumi facciali", vol. 2, chap. 29, Piccin, Padova, 1988.
- Nahas L.F., Nahas R.A.; Quemaduras electricas de los
labios y comisura bucal. Cit. Plast. lber. Latinoamer., 16: 129-34, 1990.
- Feldman J.J.: Facial burns. In: McCarthy,
"Plastic surgery", vol. 3, chap. 1, Saunders, Philadelphia, 1990.
- Luce E.A.: Electrical injuries. In: McCarthy,
"Plastic surgery", vol. 1, chap. 24, Saunders, Philadelphia, 1990.
- Neale H.W.: Electrical injuries of the hand and
upper extremity. In: McCarthy, "Plastic surgery", vol. 8, chap. 130, Saunders,
Philadelphia, 1990.
- Garriba R., Tanzarella M., Colesanto A.D., Pascone
M.: Problemi di trattamento nelle gravi folgorazioni del polso. Riv. Ital. Chit. Plast.,
15: 377-83, 1983.
- Masellis M., Conte F., Fortezza G.S.: Use of dermis
to reconstruct hand joint capsules. Ann. Plast. Surg., 9: 72-80, 1982.
- Cabanes J.: Prevention des brOlures 6lectriques.
Ann. Medit. Burns Club, 1: 38-40,1991.
|