| Ann. Medit. Burns Club - vol. VII - n. 4 - December 1994
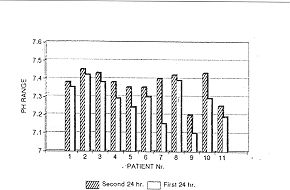
THE USE OF ALKALINE HYPERTONIC SALINE SOLUTION FOR RESUSCITATION OF SEVERE THERMALLY INJURED PATIENTS (OUR EXPERIENCE) Klein D., Millo Y., Winkler E., Shvurun A., Tzur H. Department of Plastic Surgery and Burns Unit, Sheba Medical Center, Tel-Aviv University, Sackler School of Medicine, Israel SUMMARY. Eleven severely burned patients were resuscitated in our bum intensive care unit last year. They were treated in the first 48 hours post-bum with alkaline hypertonic saline solution. Haemodynamic parameters, electrolytes, arterial blood gases and the general outcome were assessed in the first seven days. Compared to our previous experience with isotonic saline solution we concluded that better results were achieved with hypertonic crystalloids during the resuscitation period. We noticed fewer haemodynamic disturbances as well as an improvement in the prevention of tissue oedema. By using continuous infusion of sodium bicarbonate we managed to prevent the metabolic acidosis usually seen in the first 24 hours. All the patients were successfully resuscitated by this method. In the past 40 years there has been a significant decrease in mortality following major thermal injury. Understanding of the pathophysiology of thermal injury during the acute phase has improved our ability to prevent hypovolaemic shock in the first 24-48 hours (1, 2, 3, 4, 5, 6). Although many regimens have been proposed, each has its limitations and complications. Hypertonic saline solution (HSS) formulae were used for the treatment of hypovolaemic shock in the attempt to diminish the large volume of fluids which are needed for resuscitation. Monafa et al. (7) and Shimazak et al. (8) promoted the use of hypertonic lactate saline (HLS) for the resuscitation phase in acute severe thennally injured patients. This results in equally effective resuscitation with a smaller fluid requirement. The constant observation of metabolic acidosis in the acute phase induced us to use continuous infusion of sodium bicarbonate added to HSS. A retrospective analysis is presented of the observation of eleven severe thermally injured patients. Methods Eleven patients aged 20-40 years, weight 60-80 kg, suffering from second- and third-degree thermal bums in 40%-95% total body surface area (T13SA), were included in this study (Table 1). All the patients were monitored hourly after insertion of a nasogastric tube, urinary catheter, arterial catheter and endotracheal tube (when needed). Haemodynarnic monitoring covered blood pressure, pulse rate, urinary output (Table II), plus blood electrolytes: Na, K, Cl, and arterial blood gas tests (pH) (Figs. 1, 2). Daily chest X-rays were performed in the first week of hospitalization. Resuscitation started promptly, based on our formula (electrolyte profile: Na 270 meq/1, 1IC03 37 meq/1, pH injury 7.82. The volume of HSS was based on the guideline equation of 2.5 ccAg/%T13SA and changed as needed in order to maintain normal haemodynamic parameters. The total daily intake (Table I) and total daily output, together with peripheral oederna and pulmonary oedema, were observed, as well as the general outcome.
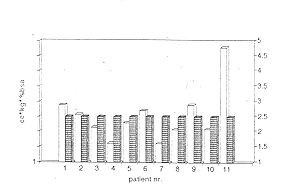
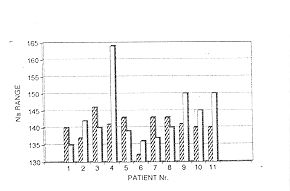
Results As said, all the patients were succesfully resuscitated. Total liquid intake according to TBSA/leg is shown in Table I, and the difference between estimated fluid needs and real intake is shown in Fig. 3. Haemodynamic monitoring showed diastolic blood pressure ranges between 60 and 95 mm Hg in the first 24 hours and between 60-80 min Hg in the following 24 h. Systolic blood pressure was between 80 and 170 Trim Hg in the first 24 hours and between 85 and 170 min Hg in the following 24 h. The pulse rate ranged between 70 and 150/min in the first 24 h and between 110 and 140/min in the following 24 hours. Urinary output ranged between 44 and 130 ml/h in the first 24 h and between 65 and 120 ml/h in the following 24 h. Sodium concentration (Fig.2) was between 140 and 150 meq/1, with the exception of one patient who had a test result of 164 meq/1 which obliged us to interrupt HSS infusion and change to Ringer's lactate solution for two hours. Blood pH was maintained between 7.18 and 7.4 in the first 24 h (Fig. 1) and between 7.40 and 7.49 in the following 24 h. Peripheral oedema and pulmonary oedema were significantly less marked than we were accustomed to seeing in patients resuscitated with isotonic crystalloid or colloid formulae. Discussion During the first hours following thermal injury there are considerable changes in the microcirculation of burn wounds. There is a loss of endothelial integrity with a massive flow of electrolytes and proteins to the extravascular space, trapping a large volume of intravascular fluids (3). This is the main cause of the hypovolaemic shock observed in the first 24 h. After approximately 12 h the endothelial gaps created by vasoactive mediators are resolved, causing slow inflow of fluids to the intravascular space. For this reason colloid therapy in the first hours of resuscitation aggravates burn wound oedema and the best results are therefore achieved with hypertonic saline solutions. We found that isotonic formulae require large amounts of fluids for resuscitation, causing peripheral oedema and pulmonary congestion. With a hypertonic crystalloid solution fewer fluids were required, resulting in less peripheral oedema and pulmonary congestion, while at the same time maintaining greater intravascular volume and lessening the risk of hypovolaemic shock. By constantly adding bicarbonate to the formula we were more successful in overcoming the metabolic acidosis that tends to develop in the first 48 hours of burn injury. Careful monitoring of the blood electrolytes prevents an inappropriate increase in sodium concentration. We regard the alkaline hypertonic saline solution formula as a good approach to prevent complications in severe thermally injured patients in the first 48 hours. RESUME. En 1993 les auteurs ont réanimé dans leur service de réanimation onze patients sévèrement brûlés. Les patients ont été traités dans les premières 48 heures après la lésion avec la solution hypertonique de sel alcalin. Les paramètres hémodynamiques, les électrolytes, les gas du sang artériel et le résultat général ont été évalués dans les premier sept jours. Par rapport à leur expérience précédente avec la solution isotonique de sel les auteurs ont conclu qu'il ést possible d'obtenir des résultats meilleurs avec les cristall6fdes hypertoniques pendant la période de réanimation. Ils ont noté un nombre inférieur de problèmes hémodynamiques et une amélioration de la prévention de l'oedème tissulaire. Utilisant l'infusion continuelle de bicarbonate de soude ils sont réussis à prévenir l'acidose métabolique que l'on observe normalement dans les premières 24 heures. Grâce à cette méthode tous les patients ont été réanimés avec succès. BIBLIOGRAPHY
THE INTERNATIONAL CONFERENCE ON
DISASTER AND EMERGENCY MEDICINE The Conference programme will include: a wide variety of seminars allowing participants to tailor the curriculum to their specific interest International faculty. All considered experts in their field Simultaneous translation in English and Chinese of all lectures and conference materials Presentation of scientific papers for international publication Trade show and exhibit Special classes on "How to do business in China" Numerous social functions to allow people to meet in an informal atmosphere Opportunity to explore and learn about '7raditional Chinese Medicine": acupunture, oriental massage, herbal medicine, etc. Optional social function for accompanying spouses and post-conference For further information contact: |