| Ann. Medit. Burns Club - vol. VII - n. 4 - December 1994
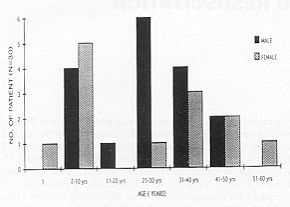
THE CONSTANT FACTOR FOR FLUID RESUSCITATION IN MAJOR BURNS Bang R.L., Ghoneim I.E. Faculty of Medicine, Kuwait University, Kuwait SUMMARY. Thirty patients (17 males, 13 females) with ~~30% T13SA burns admitted to the intensive care unit at Ibn Sina hospital, Kuwait from December 1991 to April 1993 were studied. The mean age was 24 years (range 6 months to 60 years), Twenty-five patients had sustained flame burns and five had suffered scalds. The percentage T13SA burned ranged from 30 to 85% with a mean of 55%. Resuscitation started with the Parkland formula (constant factor 4 ml/kg/%) adjusted to maintain urine output at around 1 ml/kg/hr. The evaluation of the first 24 hours' fluid requirement necessary for successful resuscitation revealed the constant factor of 3.8 ml/kg% (range 2.4 to 6.8). Among children it was constantly above 4 ml/kg/% (mean 4.8), while in adults it was always below 4 ml/kg/% (mean 3.3). The aetiological factor and burn depth did not influence the amount of fluid required for resuscitation, whereas inhalation had some effect. Ringer's lactate solution is recommended for initial resuscitation at a rate of 3 mlIkg1% burn in adults and 5 ml/kg/% in children. Introduction The increased capillary permeability due to burns causes plasma loss resulting in hypovolaemic shock. Proper treatment of the impending burn shock is clearly critical to the survival of the victim of a major thermal injury. The concept of intravenous fluid resuscitation to treat burn shock was first introduced and promoted in the late 1800s and early 1900s by Neiss (1880), Brown (1896), Tommasoli (1897), Parascandolo (1901) and Sneve (1905) (1, 2, 3, 4). Even then, until the 1940s hypovolaemic shock and shock-induced renal failure were the leading cause of death following burn injury. Today, with our current knowledge of the massive fluid shifts and vascular changes that occur during burn shock, morbidity and mortality related to burn-induced volume loss have decreased considerably (5). The resuscitation of major burns involves the administration of large volumes of fluids calculated on the basis of burn surface area and body weight, and frequently adjusted according to monitored clinical indices. It has been much debated whether to use crystalloid or colloid fluid but it is now well established that efficient fluid administration diminishes the frequency and severity of complications, and thereby results in a reduction in mortality. As our knowledge of burn pathophysiology expands, old tenets are modified or supplanted. However, numerous formulae for fluid resuscitation - Evans, 1952; Brooke, 1966; Parkland/Baxter, 1974; Muir and Barclay, 1974 (6, 7, 8) - still remain. These formulae vary both in the type of solution used and in the quantity administered. They are derived as a mean of the volumes used in large numbers of successfully treated patients, and therefore they do not necessarily apply to every particular patient being treated. The successes achieved have in some way slowed down the search for new therapeutic solutions in the light of the fact that the various researchers using different solutions have reported satisfactory results with statistically comparable survival rates (9, 10). In spite of the numerous formulae the quest continues for a constant factor (ml/kg/%) for fluid administration to patients in burn units, as climatic conditions differ from place to place and the response behaviour of each ethnic group also varies. Material and methods The ICBU (Intensive Care Bum Unit), formerly at Ibn Sina Hospital and now at the AI-Babtain Centre for Plastic Surgery and Bums, caters for major and complicated burn patients in Kuwait. country. From December 1991 to April 1993, 85 patients were admitted to the ICI3U. The total burn surface area (T13SA or % burn) was estimated by the Lund and Browder method. Twenty patients had less than 30% T13SA burn and therefore did not meet the inclusion criteria, while five patients who had over 90% TBSA burns were not actively resuscitated. Out of 60 patients with 30-90% T13SA burns, 30 who arrived at our centre within one hour post-burn were included in the study. These consisted of 17 males and 13 females (Fig. 1) with a mean age of 24 years (range 6 months to 60 years). Twenty-five of them had sustained flame burns and five had suffered scalds. The TBSA burn ranged from 30% to 85% with a mean of 55%. An indwelling urethral catheter was inserted to monitor hourly urine output. Body weight was recorded on admission and checked every day during the resuscitation period. In accordance with our protocol (Table I) crystalloid resuscitation with Ringer's lactate was started in all cases based on the constant factor (CF) 4 (Parkland formula - 4 mI x body weight in kg x % TSBA burn/24 h) and subsequently adjusted to maintain a urine output of 1 ml/kg body weight/h.
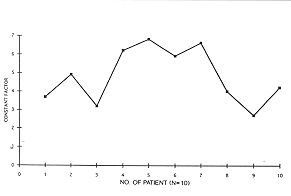
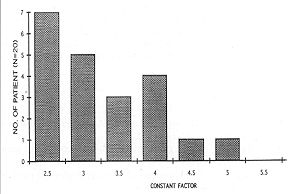
The other parameters used for monitoring the adequacy of fluid administration were vital signs (heart rate, blood pressure, respiration rate and temperature), clear sensorium, CVP and blood gases. Colloids were given at a rate of 0.5 ml/kg body weight/h after the first 24 hours postburn. The total fluid required for each patient for the first 24 hours (Ist post-burn day) period formed the basis for the CF calculation, as follows. Adequate urine output, stable vital signs, clear sensorium, normal blood gases and stable CVP throughout the course of treatment were regarded as successful resuscitation. Death during the first week post-burn was considered a failure of the treatment. Results The various data for children and adult patients are depicted in Tables II and III. All patients had successful resuscitation and no death occurred during the first week among the patients studied. The CF calculated for all patients shows a range of 2.8 to 6.8, with a mean of 3.8. However, if taken separately for adults and children (Fig. 2), the CF is consistently higher (mean 4.8, range 2.7 to 6.8), while in adults (Fig. 3) it is consistently lower (mean 3.3, range 2.5 to 5.2), suggesting that a C17 of 5 for children and 3 for adults is much more appropriate. The mean urine output was 1 ml/kg/h in adults and 1.4 ml/kg/h in children. A mean body weight increase of 8.0% in children and 11.0% in adults was observed after 24 hours. The aetiology and the depth of the burn did not influence the fluid requirement but inhalation injury had some effect. Two adult patients whose C17 was more than 4 had inhalation injury. No inhalation injury was detected among children. Three patients died, two adults (patients 3 and 11 in Table III) with 65% burns on days 25 and 66 post-burn and one child (patient 8 in Table II) with 85% burns on day 40 post-burn. They had been successfully resuscitated and their deaths were due to septicaemia and related causes at a much later date.
Discussion The aim of fluid resuscitation in burn patients is the prev.ention of uncompensated shock, and a vigorous approach to fluid therapy is required to achieve it. The fluid loss in burns patient can be predicted in a general way based on the burn surface area and the body weight. Taking this into consideration the first formula was devised in 1952 by Evans et al. (6) with a 1: 1 ratio of crystalloid to colloid. This was later changed to a 3:1 ratio by Reiss et al. in 1953 (11). There then followed a trend to abandon plasma altogether in the first 24 h, on the basis of the results of numerous studies (9, 12, 13) although this resulted in greater fluid requirements and increased oedema. In 1926 Davidson (14) was among the first to recognize the central role played by the sodium/potassium pool and the contribution of the Na+ ion in the intra- and extracellular distribution of electrolytes and water. This led to the differentiation in the conception of the administration of crystalloid solution in the initial period of burn shock resuscitation. None of the initial fluid resuscitation programmes of burns available today is optimal as regards volume, composition and infusion rate, although the total fluid requirements of the burn patient is usually between 2 to 4 ml/kg/% burn (15). The goal of burn resuscitation is to maintain adequate tissue perfusion and to prevent hypovolaemia. The purpose of a fluid resuscitation formula is not to deliver a strictly calculated volume of the specified fluid over a given time interval. When properly used these formulae provide a "guideline" for fluid resuscitation. Almost every author writing on the subject has acknowledgCd the variability of ifidividual patient fluid requirements (5, 12, 16, 17, 18, 19, 20, 21, 22, 23).
Crystalloid, in particular Ringer's
lactate solution with a sodium concentration of 130 meq/1, is the most popular
resuscitation fluid based on the Parkland formula (4 ml/kg% burn) (7, 12, 13, 15, 19, 21)
and it is widely used. In our Centre it is administered because it is simple, low cost,
safe and gives a satisfactory response in most patients. Monitoring is easily carried out
by measuring hourly urine output: an output in excess of 1.5 ml/kg/h is due to
overtransfusion (24). RESUME. Les auteurs ont étudié trente patients (17 mâles et 13 femelles) atteints de brûlures en >30% de la surface corporelle totale hospitalisés dans le service de réanimation à l'hôpital Ibn Sina, Koweït dans la période décembre 1991/avril 1993. L'âge moyen était 24 ans (variant entre 6 mois et 60 ans). Vingt-cinq patients avaient été atteints de brûlures par flammes et cinq d'ébouillantements. Le pourcentage de la surface corporelle brûlée totale variait entre 30 et 85%, avec une moyenne de 55%. La réanimation commençait avec la formule de Parkland (facteur constant 4 ml/kg/%) adaptée pour maintenir une production urinaire d'environ 1 ml/kg/%. L'évaluation des besoins de liquides dans les premières 24 heures nécessaires pour une réanimation efficace a révélé le facteur constant de 3,8 ml/kg/% (variation entre 2,4 et 6,8). Pour les enfants le facteur constant était toujours plus de 4 mllkgl% (moyenne 4,8) et pour les adultes toujours moins de 4 ml/kg/% (moyenne 3,3). Le facteur étiologique et la profondeur de la brûlure n'avaient aucune influence sur la quantité des liquides nécessaires pour la réanimation, mais l'inhalation produisait un certain effet. Les auteurs recommandent l'emploi de la solution de lactate de Ringer pour la réanimation initiale dans la mesure de 3 ml/kg/O/o de brûlure dans les adultes et de 5 mllkgl% dans les enfants. BIBLIOGRAPHY
G. WHITAKER INTERNATIONAL BURNS
PRIZE - PALERMO (Italy) By law n. 57 of June 14th 1983
the Sicilian Regional Assembly authorized the President of the Region to grant the
Giuseppe Whitaker Foundation, a non profit-making organization under the patronage of the
Accademia dei Lincei with seat in Palermo, an annual contribution for the establishment of
the "G. Whitaker International Bums Prize" aimed at recognizing the activity of
the most qualified experts from all countries in the field of burns pathology and
treatment. Michele Masellis M.D., |