| Ann. Medit. Burns Club - vol. V11 - n. 4 - December 1994
PRESSURE THERAPY IN THE TREATMENT OF ADVANCED POST-BURN
HYPERTROPHIC SCAR: A COMPARATIVE STUDY OF CLINICAL EVALUATION, PHOTOGRAPHY AND
ULTRASONOGRAPHY
Kaya L*, Kivang K*, Dalay W, AcartOrk S.*, Atila
E**
* Division of Plastic Surgery, University of
Qukurova Medical School, Adana, Turkey
** Division of Diagnostic Radiology
SUMMARY. Eleven bum patients
are presented who were treated with pressure garments. The changes in hyper-trophic scar
thickness were followed by means of clinical evaluation, photography and high-resolution
ultrasonography (USG) in our Bum Unit in 1990-1993. Patients were selected from those who
had palpable scars and were late for pressure treatment. The custom-made pressure garments
(JuzoHelastic Cotton, Germany) were worn by the patients for about eight weeks after the
burn wound had healed. Changes in scar thickness were measured by ultrasonography before
treatment and at three-monthly intervals during pressure therapy. We concluded that
pressure treatment can control advanced scars that were late for treatment. Changes in
scar thickness can be objectively demonstrated better by USG than by clinical evaluation
and photography.
Introduction
Hypertrophic scars are frequent
sequelae of burn injuries. This condition can be prevented and controlled by means of
pressure garments, the pressure of which can be controlled (1, 2, 3, 4).
Pressure treatment is usually performed by applying an elastic garment to the surface of
the scar. The general view is that pressure treatment should be applied early -preferably
two weeks after healing of the burn wound and the skin-graft areas. It has been suggested
that the garments should be worn 24 hours a day except for short periods for hygienic
purposes. The treatment should be continued for at least nine months and if scarring
recurs, it is necessary to resume treatment. For effective treatment, a pressure ranging
from 18.4 to 32.2 mm Hg should be applied (1, 5).
The many methods for following the progress or maturation of a scar include scar
elastometry, negative imaging, photography, biopsy and clinical evaluation (6).
Highresolution ultrasonic scanning is also used as an objective method for detecting skin
lesion and measuring the scar thickness quantitatively (7).
In our study, palpable hypertrophic scarred post-bum patients who were late for pressure
treatment were treated with pressure garments and the results of treatment were followed
by clinical evaluation, photography and USG. The above parameters were also compared with
each other and the results were evaluated.
Materials and methods
The group in this study consisted of
11 patients treated in the Burn Unit at the University of ukorova Medical School between
1990 and 1993. The patients' mean age was 21 years (range, 7-59) and the mean body surface
area burned was 23%.
The pressure garments were custom-made (JuzoHelastic Cotton, model 3021, compression class
1). The garments were worn by patients who were late for pressure treatment for about
eight weeks after the bum wound and the skin-graft area had healed. The patients wore the
garments 24 hours a day, except for hygienic needs, and treatment continued for about nine
months.
The patients were examined clinically every month. During clinical evaluation, photographs
were taken every three months (Cannon EOS 10 camera with a 50 mm macrolens) and scar
thickness was measured by USG (GE RT 4000 Real Time Duplex Scanner).
A test scar was chosen to evaluate the results of treatment and the distances of this scar
from anatomical landmarks were recorded. Clinical evaluation, photography and USG of the
same scar were repeated every three months. The scar was clinically graded from 0-2,
according to the findings of itchiness and firmness. After photographic evaluation the
scar was measured by ultrasonography and the results obtained were evaluated in
millimetres. This procedure was performed at a frequency of 5.0-7.5 megahertz, and the
microview transducer which functioned as both sender and receiver of sound and a small gel
bath were enclosed in a plastic membrane.
Results
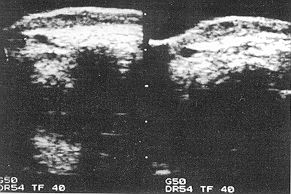
Ultrasonic scanning shows hypertrophic
scarring as an area between two hypodense lines (Fig. 1). Before initiation of
pressure treatment, USG was used to measure the scar thickness of patient #7, which was 6
mm. At this time patient #7 was grade 2, and grade 2 by clinical and photographic
evaluation (Fig.2).
 |
Fig. 1 - Ultrasonic
scan showing hypertrophic scarring as an area between two hypodense lines. |
|
 |
 |
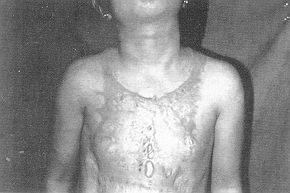
| Fig. 2 (a) - Photographic
evaluation of patient #7 before pressure treatment. |
Fig. 2 (b) -
Ultrasonic evaluation of patient # 7 before pressure treatment. |
|
 |
 |
| Fig. 3 (a) - Photographic
evaluation of patient #7 after three months of pressure therapy. |
Fig. 3 (b) -
Photographic evaluation of patient #7 after three months of pressure therapy. |
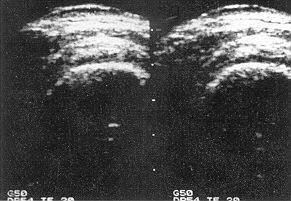 |
Fig. 3 (c) -
Ultrasonic evaluation of patient #7 after three months of pressure therapy. |
|
 |
 |
| Fig. 4 (a) - Photographic
evaluation showing results of pressure treatment in ninth month. |
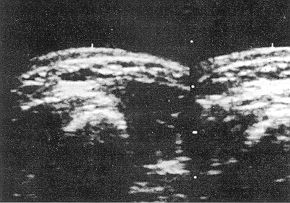
Fig. 4 (b) - Ultrasonic
evaluation showing results of pressure treatment in ninth month. |
|
US: Ultrasonography (sear thickness in mm) CE: Clinical
evaluation (scale, 0-2: itchiness and firmness0; firmness (+) = 1; itchiness and firmness
(+) = 2 PH: Photography (scale, 0-2: blistering and redness 0; blistering (+) = 1;
blistering and redness (+) = 2
thickness as measured by USG performed three months after pressure treatment was 4 mm and
at the same time clinical and photographic evaluation both gave grade 2 (Fig.3). Ultrasonic
scanning after nine months measured scar thickness as 2.0 mm, while the clinical
evaluation was grade 1, as also the photographic evaluation (Fig.4). When the
parametric findings obtained from this patient were presented in a graph (Fig.5), it
could be objectively seen that there was a clear change in scar thickness on USG
evaluation, whiIQ there was only slight change in the clinical and photographic
evaluations, in the 6-9 month period.
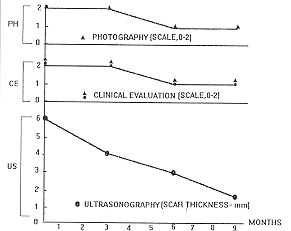 |
Fig. 5 - Graphic
display of ultrasonically measured scar thickness, photography and clinical
evaluations in patient #7 in whom pressure therapy was initiated at three-monthly
intervals. |
|
The findings obtained from the study group
were tabulated (Table I). Before pressure treatment was initiated, the scar
thickness of all the patients was grade 2. It was also grade 2 by clinical and
photographic evaluation and measured 2.2-6.0 ram by ultrasonic scanning. In the ninth
month of pressure treatment, the scar thickness of eight of the patients who were
clinically regarded as grade 0 was grade 1 on photographic evaluation and measured 1.0
trun on USG evaluation. These patients showed good clinical response, while the other
patients fared poorly.
Discussion
Hypertrophic scars characteristically
form within the first six to eight weeks after epithelialization occurs. During the
subsequent "maturation" process, which lasts two or more years, partial or
complete resolutibn typically occurs. The pressure treatment used for post-bum
hypertrophic scarring is regarded as a non-invasive method. Pressure garments not only
prevent and control scarring but also regress advanced scarring. Use of the garments
improves hypertrophic scar formation by increasing the hypoxic condition, which results in
focal degeneration of selective cells. The exact level of effective external pressure,
though usually taken as being approximately that of arterial capillary pressure (24 mm
Hg), has not been scientifically demonstrated (1).
In this study group we applied a pressure range of 18 to 32.2 turn Hg. Analysis of the
patients showed a good clinical response in 72.7% of the cases and a poor response in the
others. These rates are consistent with those of previous studies (1, 4, 8).
It is clinically important to determine scarring and regression objectively in clinically
objective terms. For this purpose photography and ultraphonographic scanning are used (9).
In our study, we were able to measure objectively the full thickness of scarring by means
of USG. With other methods, it is not possible to measure scar thickness objectively.
Measurement of scar thickness by USG is a simple method, and as it is easily tolerated by
the patients it is useful during other scannings. Another advantage is that it measures
completely both the visible and the invisible sides of the scar. To eliminate measurement
errors, the highest and the lowest measurements should be determined and the mean
calculated for the evaluation.
The clinical progress or maturation of the scarring can be evaluated by means of clinical
evaluation and photography. Small changes in scarring may not be evaluated by these
parameters. Normally, in the treatment protocol, there are no objective methods for
comparing scarring changes.
We have found that very good results can be obtained by pressure garments in advanced
post-burn scars. We followed the results of our treatment protocol by scanning scar
thickness. In our opinion, high-resolution ultrasonic scanning is a simple, noninvasive
and objective method for demonstrating changes in scar thickness.
RESUME. Les auteurs
présentent onze patients brûlés traités avec les vêtements compressifs. Les
modifications de l'épaisseur des cicatrices hypertrophiques ont été suivies par
l'évaluation clinique, la photographie et le balayage ultrasonique (USG) à haute
résolution dans notre Service de Brûlures dans les années 1990-1993. Les patients ont
été sélectionnés entre ceux qui avaient des cicatrices palpables et étaient en retard
pour le traitement de pression. Les vêtements compressifs faits sur mesure (Juzo-Helastic
Cotton, Germanie) ont été portés par les patients pour environ huit semaines après la
guérison de la brûlure. Les changements de l'épaisseur de la cicatrice ont été
misurés par PUSG avant le traitement et à intervalles de trois mois pendant la thérapie
compressive. Nous avons conclu que la compression peut contrôler les cicatrices avancées
en retard pour le traitement. Les modifications de l'épaisseur des cicatrices peuvent
être objectivement mieux démontrées par FUSG que par l'évaluation clinique et la
photographie.
BIBLIOGRAPHY
- Baur P.S., Larson D.L., Stacey T.R. et al.:
Ultrastructural analysis of pressure-treated human hypertrophic scars. J. Trauma, 16: 958,
1976.
- Kischer CW., Shetlar M.R., Shetlar C.L.: Alteration
of hypertrophic scars induced by mechanical pressure. Arch. Dermatol., I 11: 60,1975.
- Larson D.L., AbstoD S., Evans E.B. et al.:
Techniques for decreasing scar formation and contractures in the burned patient. J.
Trauma, 11: 807,1971.
- Leung P.C., Ng M.: Pressure treatment for
hypertrophic scars.Burns, 6: 244, 1980.
- Larson D.L., Abston S., Willis B. et al.:
Contracture and scaf formation in the burn patient. Clin. Plast. Surg., 1: 653, 1974.
- Alm S.T., Monafo W.W., Mustoe T.A.: Topical silicone
gel for the prevention and treatment of hypertrophic scar. Arch. Surg., 126: 499, 1991.
- Alexander 11, Miller D.: Determining skin thickness
with pulsed ultrasound. J. Invest. Dermatol., 72: 17, 1979.
- Cheng J.C.Y., Evans J.H., Leung K.S. et at.:
Pressure therapy in the treatment of post-bum hypertrophic sear - a critical look into its
usefulness and fallacies by pressure monitoring. Burns, 10: 154, 1984.
- Bartell T.H., Monafo W.W., Mustoe T.A.: A new
instrument for serial measurments of elasticity in hypertrophic scar. J. Bum Care
Rehabil., 9: 657, 1988.
THE 9TH WORLD CONGRESS ON
EMERGENCY AND DISASTER MEDICINE
will be held from 28 May to 2 June 1995
in Jerusalem, Israel
The preliminary scientific programme includes:
Different disasters and man-made accidents
Cooperation and coordination between all participating agencies, bodies and organizations
at the disaster site
Education of the general public
Exhibitions including audio and visual means, computer self teaching program in rescue
techniques, etc., to be presented at the venue
For further information contact:
Secretariat: 9th World Congress on Emergency and
Disaster Medicine
P.O. Box 50006
Tel Aviv 61500, Israel
Phone: 972 35140014
Fax: 972 35175674/660352
|