| Ann. Medit. Burns Club - vol. VIII - n. 1 - March 1995
EXTENSIVE GRANULOMA PYOGENICUM COMPLICATING SEVERE BURNS
Shlash S., AI-Jalsi L, Somorin A.
Departments of Surgery and Medicine, Armed Forces
Military Hospital, Tabuk, Kingdom of Saudi Arabia
SUMMARY. A six-year-old girl, admitted over
a seven-montb period with 70% tbird-degree bums to the Burns Unit of a tertiary Saudi
Arabian medical centre, developed an unusual form of histologically confirmed, multiple,
rubbery, widespread, vascular, giant-sized granuloma pyogenicum. Despite the corporeal
severity of the flame bums accident and the benign cutaneous neoplasm, the patient made an
uneventful recovery after multiple sessions of cryotherapy, meshed partial-thickness skin
grafting, multiple intravenous antibiotics, albumin, blood and other fluids.
Introduction
Granuloma pyogenicum is a benign
vascular neoplasm of regenerating capillaries, primary to a traumatic ulcer of the skin
and/or mucous membrane or secondary to a chronic cutaneous lesion where the skin surface
has been damaged or infected, e.g. after pustular acne vulgaris. However, when such a
condition fonns a foamy, red-balloon, "Michelin tyre" appearance with satellite
lesions, it becomes a clinical diagnostic masquerade. This paper describes such a clinical
problem.
Case report
A six-year-old Bedouin girl sustained
kerosene bums to almost the entire body skin surface. After local first-aid measures
applied at her home she was seen at the nearest medical facility, from where she was
referred on 12 November 1992 to our hospital. Her family resides in the desert and the
girl had no relevant family, dermatological, obstetrical or surgical history.
On examination, she weighed 16.05 kg and presented about 70% full-thickness burns in the
left leg, right arm, axillae and antero-medial aspects of the chest. Other sites affected
were: chest and abdomen (12%), upper limbs (13%), lower limbs (23%), buttocks (5%), back
(12%), head (1%) and genitals (1%). All these areas were inoculated with tender, sessile,
pedunculated, polypoid, papular, soft, rubbery, wet, red and vegetative swellings. The
patient was hairy (for her age), pale, pyrexial and miserable-looking (Figs. 1, 2, 3).
The clinical picture was as follows: Hb = 9.7 gm%, Het = 80.5, platelets = 217 x 109/1,
WBC = 15.7 x 109/1, HIV negative, hepatitis negative. Skin swab grew
methicillin-resis-tant Stapkylococcus aureus sensitive to vancomycin, clindamyein
and rifampicinum. Urine culture grew Providencia rettgeri and E. coli
sensitive to ciprofloxacin. Blood group: 0 Rh positive, AST, ALT = NAD. Albumin = 18 g11,
total protein = 46 g11. Creatinine = 33 pmol/1, urea 7.3 mniol/1. Alkaline phosphatase:
220 u/1 sodium, 133 mmol/1, potassium, 3.9 mmol/1. Blood culture: Staphylococcus organisms
sensitive to vancomycin and ciprofloxacin. Urine culture: over 100,000 col/ml of E.
coli and Pseudomonas aeruginosa sensitive to gentamycin and ciprofloxacin.
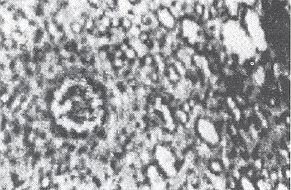
Skin biopsy revealed a pedunculated skin tissue with
characteristic crust and birefringent connective tissue fibres. There was a proliferation
of the endothelial cells and numerous capillaries. At the base of the tissue the rete pegs
were prominent while there was abundance of hair follicles with cyst-like horn structures.
The histological diagnosis was ulcerated granuloma pyogenicum.
Progress report
About five weeks after admission
the patient was observed to have developed ball-like, rubbery, soft, polypoid nodules
vegetating from the red raw painful burned areas. The patient was subjected to multiple
sessions of blood transfusion, albumin infusion, variously bacteriologically dictated
antibiotics, cryotherapy and serological monitoring of drug blood levels, e.g. of
vancomycin. As the patient lived at some distance from the hospital, and because of the
unavailability of her own skin for grafting, she had multiple sessions of grafting during
her prolonged hospital stay. On 20 February 1993 she was subjected to partial thickness
mesh-grafting and removal of some granulation tissue of the right arm, axilla and chest,
and on 28 March, 25 April and 19 May 1993 to shaving of exuberant granulating tissue from
the supra- and infra-umbilical and inguinal areas. The patient had a skin graft mesh 1-3
(taken from both legs and left forearm) applied to the gluteal and popliteal regions and
the anterior and lateral chest wall.
Cryotherapy was performed using liquid nitrogen at 196 'C followed by Fucidin cream
dressing with pressure bandaging. The patient made an uneventful recovery and was
discharged on 7 August 1993. She continues to enjoy good health up to the time of writing.
Discussion
Granuloma pyogenicurn (GP) is a
cutaneous, vascular or red-coloured, papular, nodular condition that may occur either
primarily or secondarily to a healing cutaneous swelling. It is a benign vascular tumour
of the skin. Ro (1) described its pathogenesis, clinical features and mode of treatment.
Subsequently Fromm and Asaad (2) amplified this further, maintaining that GP is a
conglomeration of regenerating capillaries that has been associated with secondary
infection even though no infective agent has been identified as a primary cause. Probably
overgranulation of these tissues causes the exuberant growth of the tumour and this
probably exposes its surface to recurrent or frequent traumatization.
Despite this macroscopic picture of GP, ultrastructural studies have shown that there is
endothelial cell-proliferation with widening of the oedematous intercellular spaces and
new vessel formation. Hence Marsch (3) felt that "capillary haemangioma" was a
better term for GP. The tendency of GPs to bleed quite easily on slight trauma probably
also supports this idea.
Cases of GP usually develop some four to five weeks after an initial primary skin lesion,
as in our patient. But the satellite and the widespread distribution, as shown in the
figures, are unusual and may create a diagnostic dilemma because the rubbery, vascular,
nodular morphology simulates Kaposi's sarcoma, fibroma, epiloia of tuberous sclerosis,
haemangioma, angiosarcoma, keloids, cutaneous leishmaniasis, keratoacanthoma and
angiofibroma. However, the association of traumas in GP excludes these conditions (except
keloids).
However, in rare cases, a melanotic malignant melanoma may mimic GP, although the latter
is commoner in the head and trunk while the former is seen in all areas but seldom in the
trunk (4).
The wide distribution of GP in the patient described here, coupled with the severity of
the bums, aggravated the prognosis. Forjouh and Smith (5) have shown that the fatality
rate in bums is affected by the extent and depth of the lesions and by the delay in
initiation of treatment, but this patient was able to survive because therapy was
initiated immediately (i.e. a few hours) after the accident. This therapy consisted of
supportive intravenous fluids (5% albumin, blood, dextrose-saline),
bacteriologicallydetermined antibiotics and intermittent surgical repairs with grafting of
the affected skin.
Various modalities of treatment have been explored in the management of GP. Fong et al.
(6), working in Singapore over an 18-month period, studied 41 GP patients with various
lesions including capillary haemangiomas, cherry angiomas, telangiectasis and spider
angiomas. Most of the patients responded very well to argon laser therapy, with few
complications. Dejonckere et al. (7) reported exuberant GP as a post-surgical complication
of endoscopy laser surgery for laryngeal papillornatosis. In contrast, Zaynoun et al. (8)
treated most cases of GP surgically but reported a recurrence even after
electrocoagulation. This surgical regime was also practised by Sen (9) in patients with
palpebral, pedunculated conjunctival GP, although this method of treatment was
complemented by diathermy.
Granuloma pyogenicum can be successfully treated only by repeated cryotherapy integrated
with bacteriologically defined antibiotic cover, as in our patient. It is therefore
suggested that cases of GP occurring in exposed parts should be treated exclusively with
electrocoagulation with or without antibiotic therapy.
Acknowledgement
We would express our appreciation for the services and
support of the nursing staff, the Dermatology and Burns Unit and the Communications
Department, Armed Forces Military Hospital, Tabuk. The secretarial service of Ms Cecile M.
Pefia is gratefully acknowledged.
RESUME. Une enfant âgée de
six ans atteinte de brûlures de troisième degré dans 70% de la surface corporelle et
hospitalisée pendant sept mois chez le Service de Brûlures d'un centre médical
tertiaire en Arabie Saoudite a commencé à souffrir d'une forme inhabituelle de granulome
pyogénique multiple, diffus, vasculaire, caoutchouteux, de taille géante et
histologiquement confermé. Malgré les problèmes présentés par la sévérité
corporelle des lésions causées par les flammes et par le néoplasme cutané bénin, la
petite patiente est guérie sans incidents grâce à une série de sessions de
cryothérapie, greffes cutanées mesh à épaisseur partielle, antibiotiques intraveineux
multiples, albumine, sang et d'autres liquides.
BIBLIOGRAPHY
- Ro Byung: Granuloma Pyogenicum. Int. J. Derm., 25:
1634-5, 1986.
- Fromm L., Asaad D.: Granuloma pyogenicum. In:
"Textbook of Dermatology in General Medicine" (3rd ed.), pp. 1063-4, Fitzpatrick
T. B. et al. (Eds.), McGraw-Hill Book Company, New York, 1987.
- Marsch W. C.: Ultrastructure of eruptive capillary
haemangiorna.Hautarzt, 35: 92-6, 1984.
- Bassakas 1. D., Kuhnert A., Diepgen T. J., Hornstein
0. P.: Clinically relevant differences between a melanotic, malignant melanoma and
granuloma pyogenicum. Dermatologica, 182: 81-4,1991.
- Forjouh S. N., Smith G. S.: Case-fatality rate by
body part affected and trends in hospitalised bums in Maryland. 1981-90. Burns, 19..
387-90, 1993.
- Fong P. H., Chan H. L., Tan W.: Initial experiences
with the argon laser in cutaneous vascular lesions. Annals of the Academy of Medicine,
Singapore, 53: 17, 498-501, 1988.
- Dejonckere P. H., Franceschi D., Scholtes J. L.:
Extensive granuloma pyogenicum as a complication of endolaryngeal argon laser surgery.
Lasers in Surgery and medicine, I 1: 41-5, 1985.
- Zaynoun S. T., JuIjulian H. H., Kurban A. K.:
Pyogenic granuloma with multiple satellites. Are. Derm., 109: 689-91, 1974.
- Sen D. K.: Granuloma pyogenicum of the palpebral
conjunctiva. J. Paediatric Opthalmology and Strabismus, 19: 112-4, 1982.
'95
INTERNATIONAL CONFERENCE ON DISASTER AND EMERGENCY MEDICINE
will be held from 18 to 20 April 1995
in Shanghai, China
The Conference programme will include: a wide
variety of seminars allowing participants to tailor the curriculum to their specific
interest International faculty. All considered experts in their field Simultaneous
translation in English and Chinese of all lectures and conference materials Presentation
of scientific papers for international publication Trade show and exhibit Special classes
on "How to do business in Chiria" Numerous social functions to allow people to
meet in an informal atmosphere Opportunity to explore and learn about '7raditional Chinese
Medicine": acupunture, oriental massage, herbal medicine, etc. Optional social
function for accompanying spouses and post-conference
For further information contact:
Asia ICODEM - Shanghai Medical Aid Center
68 Manning Road - Shanghai 200080, China
Tel. 8621/329/1395 - Fax 8621/320/7612
America S. Francisco Ambulance Service Inc.
Europe 2829 California Street, S. Francisco, CA 94115
Tel. 415/922/9400 - Fax 415/931/0196 |
|