| Ann. Medit. Burns Club - vol. VIII - n. I - March 1995
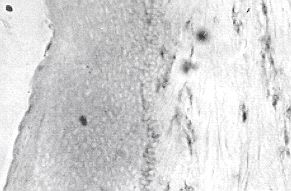
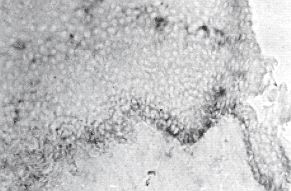
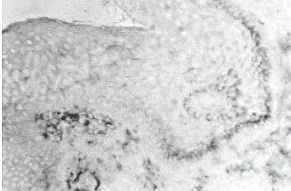
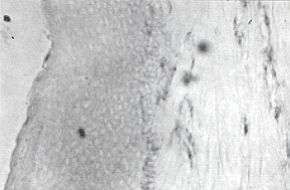
THE ROLE OF TNF ALPHA AND BETA CYTOKINES IN SCAR HYPERTROPHY IN BURN PATIENTS: AN IMMUNOHISTOCHEMICAL STUDY Castagnoli W, Stella W, Magliacani W, Richiardi R** * Centro Grandi Ustionati, CTO, Torino, Italia SUMMARY. The pathogenetic factors involved in the development of hypertrophic scarring are still to some extent unknown. It has recently been found that biopsies of hypertrophic scars reveal an anomalous behaviour of molecules activating the immune system. A significant association has also been observed be , tween class 11 histocompatibility leucocyte antigens (HLA) and the formation of hyper trophic scars. This paper analyses the percentagebf cells that produce the tumoral necrosis factor (TNF) alpha and beta in hypertrophic scars, using normal scar biopsies and healthy skin biopsies as controls and following the three-stage immunoperoxidase method and specific monoclonal antibodies. The samples were initially studied in order to characterize cell infiltrates. The biopsies of hypertrophic scars showed a massive presence of infiltrating activated cells capable of producing TNF beta and IL- I beta. The percentage of cells producing TNF alpha (8~vo) was significantly smaller than that in normal scars (35.4%). The production of TNF beta was found to be substantially similar in hypertrophic and normal scars. Introduction Scar hypertrophy is one of the greatest problems in the healing of severely burned patients, conditioning their ultimate recovery and complicating and worsening the results of therapy. Progress in the physiotherapeutic and surgical treatment of scars (elastic pressure, media contact, filiform showers, skin expanders, etc.) has led to great improvements ' without however entirely eliminating the impact of this pathology on the patient and on society. Basic research in numerous fields on the aetiology of the pathology has provided only inconclusive evidence, which requires further investigation if it is to yield new concepts that may be applied also on the therapeutic level. The study of the poorly understood factors involved in the actiopathogenesis of scar hypertrophy is therefore of particular importance, and may lead to new therapeutic approaches. Clinical observations of the evolution of burn scars indicate that hypertrophy occurs from one to three months after closure of the lesions and regresses in a period ranging from a few months to a number of years. It has been suggested that temporary hypertrophies (i.e. regressing within six months) should be considered borderline phenomena (1). Attempts have also been made to use clinical and laboratory criteria to predict the regression time of persistent hypertrophies (i.e. of more than six months' duration). A retrospective survey of patients in our Centre did not yield any predictive clinical criteria regarding the evolution of scarring (2). Many researchers attribute an important aetiological role to immunological factors such as the increase in circulating immunoglobulins, Langerhans tissue cells and amoantibodies and the aberrant presence of molecules activating the immune system in pathological tissue (3, 4, 5, 6, 7). A significant association has been found between class II HLA alleles and the formation of hypertrophic scars (8). This association suggests that genes involved in the process of pathological scarring may be located in the region of the HLA chromosomes. This is also the region of the genes which codify for the tumoral necrosis factor alpha (TNF alpha) and TNF beta, which play a crucial role in the remodelling of tissue shape (10). In the light of these considerations we considered that it would be interesting to analyse the production of these cytokines in biopsies of hypertrophic scars. Patients and methods The fourteen patients (8 female and 6 male) with hypertrophic scars secondary to burns (10-40% body surface area) selected for the survey were followed up for at least a year after closure of the burns and treated with continuous pressure therapy. They presented prominent, erythematous and often painful scars with varying degrees of contracture which were judged clinically to be active lesions without any sign of regression. Biopsies (5 mm) were removed in the course of corrective surgery, immersed in OCT, frozen in cold isopentane (-70 'C) and cryostat-sliced into 5 micron sections. The serial sections were fixed in acetone for 10 min and covered with monoclonal antibodies (Table I) at optimal dilution for 45 min. After three washings the sections were incubated with anti-rat rabbit lg for 45 min. After further washings incubation was Performed with peroxidaseantiperoxidase for 60 min and then with the A.E.C. substrate (Pap three-stage immunoperoxidase method). A quantitative analysis was made by counting the marked cells in two serial sections. In the first section infiltrating cells were stained with specific antibodies and in the second with the antibody specific for TNF alpha, beta and IL-beta. The epidermis, papillary dermis and the reticular dermis were considered separate compartments. The percentage of cells positive for TNF alpha and beta was calculated as the ratio between cells marked positively with TNF alpha and beta respectively and the total number of infiltrating cells, calculated in corresponding fields in the first section of the series. For controls we used seven biopsies of normal scars and six of healthy skin obtained in similar manner from patients undergoing plastic surgery. These biopsies were processed according to the method described. Results Characterization of the infiltrates The hypertrophic scar samples constantly presented a much higher number of infiltrating cells than normal scars and healthy skin (Table II). The infiltrating cells included
Langerhans cells (C131), macrophages (CD11), T lymphocytes (CD3 + C132) and rare NK (CD56 + CD57). B lympocytes (CD22) were not observed. In hypcrtrophic scars 70% of the T cells were activated (IL-2R+, HLA-DR+) compared with 40% found in normal scars and 10% in healthy skin. Production of TNF alpha In all the samples analysed the first
section of the sequential series was stained with anti-macrophage antibodies and total T
anti-lymphocytes. These two antibodies together react with the cell types which once
activated are able to produce TNF alpha and which constitute the majority of the
infiltrates present in hypertrophic scars. The sequential section was marked with the
anti-TNF alpha antibody and the number of positive cells in corresponding fields of the
two sections was compared. No significant difference was found between the epidermis, the
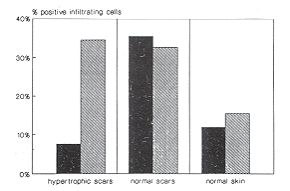
papillary dermis and the reticular dermis. All three compartments were thus considered. Production of TNF beta The same approach was used to quantify the production of TNF beta. TNF beta was produced by 37% of cells infiltrating hypertrophic scars, 30% in normal scars and 15% in healthy skin. There was a significant difference between hypertrophic scars and healthy skin (Student's ttest P < 0.0044), but there was significant difference between pathological and normal scars. Fig. 2 shows a typical result of marking. The results of TNF alpha and beta production in hypertrophic scars are summarized in Fig. 3. Discussion The above findings would suggest that
the hypertrophic scar is in an immunologically active state and that an altered production
of cytokines such as TNF alpha could play an important role in this process.
In conclusion, we would say that the
immunohistochemical method shows a low production of TNF alpha and a production of TNF
beta comparable to mature sears in burn-related hypertrophic scars. ACKNOWLEDGEMENTS. This work was sponsored by the Piedmont Foundation for Study and Research on Burns, from which C. Castagnoli received a scholarship. We would also thank G. Filogamo for his collaboration with the cryostat, G. Panzica for his advice for the realization of the quantitative procedure and G. Ponzio for the microphotographs.
RESUME. Nous ne connaissons pas avec précision tous les facteurs pathogénétiques impliqués dans le développement de la cicatrisation hypertrophique. Récemment des recherches ont montré que les biopsies des cicatrices hypertrophiques révèlent un comportement anormal des molécules qui activent le système immun. On a aussi observé une association significative entre les antigènes leucocytaires d'histocompatibilité (HLA) de classe II et la formation des cicatrices hypertrophiques. Les auteurs de cet article analysent le pourcentage des cellules qui produisent le facteur de nécrose tumorale (TNF) alpha et béta dans les cicatrices hypertrophiques, utilisant comme témoins les biopsies de cicatrices normales et de peau saine et suivant la méthode triphasée de l'immunoperoxydase et les anticorps monoclonaux spécifiques. Les prélèvements ont été étudiés initialement pour caractériser les infiltrations cellulaires. Les biopsies des cicatrices hypertrophiques montraient une présence massive de cellules activéc6 infiltrantes capables de produire TNF béta et IL-1 béta. Le pourcentage des cellules qui produisaient TNF alpha (817o) était significativement inférieur à celui des cicatrices normales (35.4%). La production de TNF béta était très simile dans les cicatrices hypertrophiques et normales. BIBLIOGRAPHY
|