| Ann. Medit. Burns Club - vol. V111 - n. 2 - June 1995
THE RHOMBOID RELEASE: A NEW APPROACH TO
THE MANAGEMENT OF DIGITAL BURN CONTRACTURES
Uzunismail k Kahveci R,
Ozdemir A, Bozdogan N ., Yuksel F.
Gulhane Military Medical Academy and
Medical School,
Hayclarpasa Teaching Hospital, Department of Plastic and Reconstructive Surgery and Burn
Centre,
Kadik6y, Istanbul, Turkey
SUMMARY.
A new approach, the "rhomboid" release, was used for chronic moderate flexion
contractures of the fingers due to burns in nine adult cases. All patients progressed well
post-operatively. The follow-up period was six months to one year without long-term
problems. As an alternative to other reconstruction methods, the procedure was found to be
versatile especially in the treatment of long-standing bum contractures limited to the
palmar skin and causing extension deficits of less than 80'. The result of the procedure
in one illustrative case is presented together with a review of the related literature.
Flexion contractures of the fingers due to
deep burns can present challenging problems. They may be limited to the volar skin or
involve deeper structures, causing severe deformity with limitation of finger movements.
Various methods have been proposed for the management of chronic flexion contractures of
the digits. These range from simple release of the contractures with graft coverage to a
number of flap procedures, including Z-plasty. When we are dealing with contracture
release, reconstruction of the secondary defects by surface covering should be evaluated
first. Unless adequate coverage is provided, many of the secondary wound healing problems
can cause residual joint contractures (1). Pre-operative tissue softening by means of
passive stretching of the contracture can sometimes be utilized as an aid to surgical
treatment.
Method
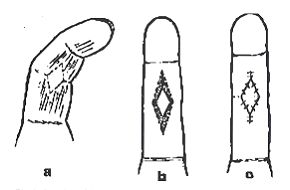
Under brachial block with tourniquet,
a 60-120' rhom~ boid incision is planned on the most prominent part of the contracture
while the finger is as far extended as possible. Incision begins from the proximal and
distal edges of the rhomboid, with the finger maintained in the extended position. The
incision is then continued to the radial and ulnar edges. When the incision is complete,
the contraction is released perpendicularly by using both faces of the blade. It is very
important to avoid horizontal undermining in order to preserve the blood supply to the
rhomboid skin island. After release of the contracture at the proximal and distal edges,
the palmar skin adjacent to the ulnar and radial edges of the rhomboid are incised 2-3 man
vertically to facilitate further release if necessary. Care is taken not to injure the
neurovascular bundle which can easily be identified under microscopic magnification.
The tourniquet is released and the rhomboid skin island is checked for its viability. The
secondary and proximal and distal palmar defects are then closed in V-Y fashion. The u1nar
and radial tongues of the rhomboid are advanced into the V-shaped defects which are
secondary to the vertical incisions on both sides, if used (Fig. ]a, b, c).
|
Fig. 1 - Drawings
of the procedure a) outline of incision b) rhomboid release (dotted area indicates the
extent of release). |
|
Case reports
We used rhomboid release in 15 fingers
of eight male and one female patients (aged 20-22 years), with moderate flexion
deformities and extension deficits varying from 40 to 80' due to burns (Table 1). We
demonstrate one example that has been documented photographically.
Case report
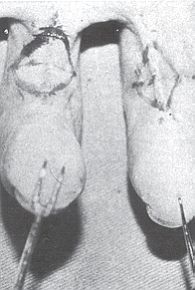
A 22-year-old serviceman (case 5) had
chronic flexion contractures, causing 50' and 60' extension deficits of the left index and
middle fingers respectively, due to flame burns sustained in childhood (Fig. 2). The
deformity followed conservative treatment which led to difficulty in using the hand, and
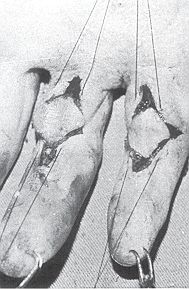
he clearly required medical treatment. He had not undergone any previous surgery. After
the contractures over the PIP joints had been released by rhomboid incisions (Fig. 3),
the secondary defects were closed in V-Y fashion. The fingers regained full extension. The
patient progressed well post-operatively and presented no problems in the one-year
follow-up period (Fig. 4).
Case |
Age |
Sex |
Involved Finger |
Extension |
Tissue gain (in
num |
|
|
|
|
No. |
|
|
Right |
Left |
deficit |
|
Prox. |
Dis. |
Total |
| |
|
|
|
|
Preop. |
Postop. |
|
|
|
1 |
20 |
m |
Index |
|
60 |
0 |
8 |
8 |
16 |
2 |
22 |
m |
Ring |
|
60 |
0 |
7 |
6 |
13 |
| |
|
|
Little |
|
60 |
0 |
7 |
6 |
13 |
3 |
22 |
F |
Middle |
|
40 |
0 |
8 |
8 |
16 |
| |
|
|
Ring |
|
60 |
0 |
6 |
6 |
12 |
| |
|
|
Little |
|
60 |
0 |
6 |
5 |
11 |
4 |
21 |
m |
Little |
|
70 |
0 |
6 |
5 |
11 |
5 |
22 |
m |
|
Index |
50 |
0 |
6 |
6 |
12 |
| |
|
|
|
Middle |
60 |
0 |
6 |
6 |
12 |
6 |
22 |
m |
Index |
|
70 |
0 |
6 |
6 |
12 |
7 |
21 |
m |
Index |
|
60 |
0 |
8 |
7 |
15 |
8 |
20 |
m |
Middle |
|
80 |
10 |
6 |
5 |
11 |
| |
|
|
Ring |
|
80 |
20 |
5 |
5 |
10 |
9 |
20 |
m |
Middle |
|
80 |
10 |
6 |
5 |
11 |
| |
|
|
Ring |
|
80 |
10 |
6 |
5 |
11 |
|
| Table 1 - Cases in which rhomboid release was
performed |
|
Discussion
Although volar contractures of the
fingers are less fre quently seen than dorsal contractures, they may nonethe less
constitute major problems. Many palm burns that heal spontaneously may continue to develop
significant scarring and eventually contractures. Chronic moderate flexion contractures of
the fingers must be regarded not only as cosmetic but also as functional problems. Such
deformities may be limited to surface problems of palmar skin or be caused by underlying
deep structures, such as vessels, nerves, tendons, joints or bones. If the deformity
involves the dominant hand, the patient may have addition al problems.
A number of methods have been developed for the treatment of digital burn contractures of
various degrees. The simplest of these would appear to be release of the contracture by
perpendicular incisions and coverage of the secondary defect by skin graft.' This method
is not however free of problems. The releasing incisions should reach as far as unscarred
tissue so that the us~fulness of residual palmar skin is maximized. Some controversy
exists concerning the use of split- or full-thickness graft after release of contractures.
Pensler et al.' advocate splitthickness graft while Jackson' prefers full-thickness graft
as this is believed to be more durable and to result in fewer recurrent contractures.
Alexander et al.' have suggested that there is no major functional difference in the use
of split- or full-thickness graft. After complete contracture release, flap coverage seems
to be the most desirable method of treatment, especially in cases where deep structures
such as tendons or joint capsules are exposed.' Pre-operative passive stretching may be
useful in all release procedures as an aid to surgical treatment.'
 |
 |
| Fig. 2 - Pre-operative
appearance of long-standing digital contractures in index and middle fingers of left hand
and drawings of incisions. |
Fig. 3 -
Intra-operative appearance of the procedure. |
|
In chronic cases with exposure of
tendons or joint capsules, the following procedures have been used: crossfinger flap,'
Z-plasty with or without accompanying skin grafts, V-shaped flap' and double opposing V-Y
flap.` In our department, multiple Z-plasty, side finger flap and five-flap Z-plasty have
all been used routinely in selected cases, in addition to the combined use of side finger
flap and cross~finger flap in severe cases.`

|
Fig. 4 -
Late results. |
|
Ex~ept for the double opposing V-Y flap
procedure, all the reconstruction procedures related to flap use have necessitated
additional grafting either for secondary defects or for coverage of flap donor areas.
We have found that rhomboid release, as named by us, is versatile and provides 5-8 mm of
tissue gain in both the distal and the proximal edges of the contracture, making a total
gain of 1-1.6 em. In the management of cases with moderate digital contractures with
extension deficits of less than 80' and with only limited volar skin, the method has
provided solid coverage without necessitating additional graft. In two cases with
extension deficit of 80', only a 10-20' deficit remained (Table I). This method has
also been found to be advantageous compared to other flap construction methods, especially
those requiring additional grafting in terms of innervation, skin texture, durability and
cosmetic appearance. It can be practised on more than one finger in the same operating
session.
We conclude that this new method can be added to the plastic surgeon's armamentarium as a
reliable and simple way of releasing long-standing contractures of the fingers.
RESUME. Les
auteurs ont utilisé une nouvelle méthode, le "dégagement rhomboïdal", pour
les contractures chroniques modérées de flexion des doigts causées par les brûlures
dans neuf cas adultes. Tous les patients ont fait de bons progrès post-opératoires. La
période de suivi post-hospitalier de six mois jusqu'à un an n'a pas présenté de
problèmes à long terme. Comme alternative à d'autres méthodes de reconstruction, cette
procédure s'est montrée très utile, particulièrement dans le traitement des
contractures de longue date dues aux brûlures limitées à la peau palmaire et qui
causent des déficits d'extension de moins de 80'. Les auteurs présentent les résultats
de la procédure dans un cas qui sert à illustrer le problème et ils passent en revue la
littérature relative.
BIBLIOGRAPHY
- Doneland M.B.: Reconstruction of the burned hand and
upper ex-trenrity. In: McCarty J.G., May J.W., Littler J.W. (Eds): "Plastic
Surgery", p. 5452, W.B. Saunders Co., Philadelphia, 1990.
- EI-0tefy M.A.: A versatile method for the release of
bum scar contractures. Brit. J. Plast. Surg., 34: 326, 1981.
- Pensler J.M., Stew4rd R., Lewis S.R., Hemdon D.N.:
Reconstruction of the burned palm: full-thickness versus split-thickness skin grafts
long-term follow-up. Plast. Reconstr. Surg., 81: 46, 1988.
- Jackson I.T.: Discussion. Plast. Reconsfir. Surg.,
68: 225, 198 1. it.
- Alexander J.W., MacMillan B.G., Martel C., Krummel
R.: Surgical correction ol'postburn flexion contractures of the fingers in children.
Plast. Reconstr. Surg., 68: 218, 198 1.
- Matthews R.N., Morgan B.D.G.: Multiple seagull flaps
for digital contractures in electric burns. Brit. J. Plast. Surg., 40: 47, 1987.
- Joshi B.B.: Percutancous internal fixation of
fractures of the proximal phalanges. Hand, 8: 86, 1976.
- Jackson I.: A method of treating chronic flexion
contractures of the fingers. Brit. J. Plast. Surg., 23: 373, 1970.
- Gibraiel E.A.: A local finger flap to treat
post-traumatic flexion con tractures of the fingers. Brit. J. Plast. Surg., 30: 134, 1977.
- Nathan P.A.: Double V-Y flap for correction of
proximal interphalangeal joint flexion contractures. J. Hand Surg., 9A: 48, 1984.
Numanoglu, A., Bas L., Celebiler
0.: Reconstruction of severe flexion contractures of the fingers by the neurovascular
laterodigital flap combined with crossfinger flap. Program and Abstracts Book, p. 226.
Presented at IPRS, Fifth Congress of Asian Pacific Section, Istanbul, Turkey, September
1989.
E.B.A.
Scientific Prize 1995
To stimulate research into the
treatment of burns, a Solvay Pharma scientific award will be presented in 1995 during the
E.B.A. conference in Verona, Italy (13-15 September 1995). Nominees are now being sought
for this prize of the European Burns Association (the E.B.A. Scientific Prize). Medical
research which has recently culminated or will soon culminate in publication in a
recognized scientific journal or in a doctoral thesis is eligible. The work must have ap
peared in the last two years and must be written in the English language.
The award will be presented by
Solvay Pharma once only and consists of a sum of money of DFL 15,000 (270,000 BEF, 6,800
ECUs, 12,300 SF). The money will be used for financing further scientific research, as the
winner sees fit. The jury will allocate the award to a physician/researcher who has been a
registered physician for no more than ten years. The winner is obliged to deliver a paper
on the winning research at the scientific meeting of the European Burns Association. This
delivery may take no more than 15 minutes. The report on the scientific research must be
supplied with a recommendation by one member of the E.B.A. and should be sent to the
secretary of the jury (five copies of each) before 15 July 1.995.
The award ceremony will take place during the 1995
E.B.A. conference in Verona on Thursday 14 September 1995.
For more information or detailed regulations, contact: The Secretary of the Jury,
P.F.J.H.A. SaIden, MD, Solvay Pharma C.J. van Houtenlaan 36, 1381 CP WEESP, The
Netherlands Phone: +31 (0)2940 77303 Fax: +31 (0)2940 80253 |
|