| Ann. Medit. Burns Club - vol. VIII - n. 3 - September 1995
A BIOSYNTHETIC SKIN SUBSTITUTE (BIOBRANE)
IN THE MANAGEMENT OF BURNS
Terr6n J., Codina J., P6rez del
Caz M.D., Safont J., Mirabet V.
Departamento de Cirugia Plàstica
y Quernados, Hospital Universitario La Fe, Valencia, Spain
SUMMARY. This
study concerns our use of a temporary skin substitute (Biobrane) in the management of
excised burn wounds (deep bums). We also use Biobrane to cover meshed autograft. It is
demonstrated that this skin substitute diminishes the healing and closing time of the mesh
and improves graft take. The use of Biobrane in autograft donor sites is also discussed.
Introduction
At present the use of a temporary skin
substitute (TSS) is an elective therapy in the treatment of full- and partialthickness
wounds affecting a large body surface area. When surgeons cannot find sufficient donor
sites for skin autografts or when it is difficult to evaluate the depth of excision, a
skin substitute has to be found. Other reasons' may be: difficult bleeding control,
excision of a massively infected burn, poor general condition of the patient, and test
graft.
The ideal properties of a skin substitute are: adherence, control of evaporative water
loss, safety (sterile, hypoallergic, non-toxic, non-pyrogenic), flexibility, durability
and stability on various wound surfaces, bacterial barrier, ease of application and
removal, availability and ease of storage, cost-effectiveness, and haemostatic efficiency.
Cultured skin is the ideal skin substitute, and will be the treatment of the future.
Long-term results',' indicate that cultured epithelial autografts regenerate a stable
normal epidermis and are capable of inducing regeneration of connective tissue
histologically indistinguishable from dermis in the process of wound healing. However,
when in vitro cultured keratinocytes have been used, the high costs and the results have
been disappointing.
Other TSS used widely at present are: skin allografts, biosynthetic skin substitutes
(BSS), and amniotic membranes. Fresh or frozen allografts, when available, are the best
choice in a temporary cover. They are rejected by the host within 14 to 21 days of
application .
Multiple synthetic materials have also been used : 4 solid silicone, plastic membranes
(polyvinyl chlorides and polyurethanes),' cotton gauze bonded to silicone, nylon mesh
bonded to silicone (Biobranc), and recently two porous copolymer layers of L-lactide and
e-caprolactone with a poly (ether-urethane) membrane dressing.
The aim of this work is to show how Biobrane is able to manage deep burns and to discuss
its use in TSS, in covering skin-meshed autografts, and in protecting skin donor sites
during healing.
Materials and methods
Biobrane, developed in 1979 by
Woodroof, consists of a custom-knitted nylon fabric mechanically bonded to an ultrathin
silicone membrane. The entire dressing is uniformly coated with collagen peptides
covalently and independently bonded to the dressing, rendering the dressing hydrophilic
and tissue-compatible.'
Case reports
Case 1
A 14-year-old Caucasian boy was admitted
to the bum centre with deep gunpowder burns affecting the thorax, abdomen and left lower
extremity (25% TBSA). He underwent an early bum excision on day 4 post-burn. The whole
excised area was covered with Biobrane and a cornpressive dressing with Furacin. This
dressing was changed every two or three days. Seven days after debridement we removed
Biobrane from the leg (Figs. 1, 2) and grafted the good wound bed with a meshed 3:1
autograft (Fig. 3). We then covered the graft with Biobrane and an occlusive
dressing (Fig. 4). We used Biobrane on the donor site (flank of the abdomen and
lower back). The thorax and thigh were not ready for grafting and we performed a second
debridement on them, even if we had observed an improvement in the bed. Fig. 5 shows
how the meshed graft was closing beneath the BSS. Ten days after grafting we removed the
Biobrane and found that the graft had completely taken and the mesh was closed (Fig. 6).
At the same time the donor site was epithelialized beneath the BSS. We grafted the rest of
the areas ten days after the first burn excision and managed them as above with the same
good results. Infection was not present anywhere under the BSS.
 |
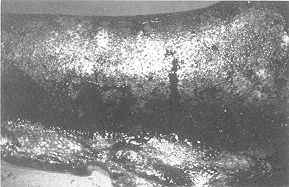 |
| Fig. 1 -
An early excised deep burn in the leg. Biobrane covering the wound. |
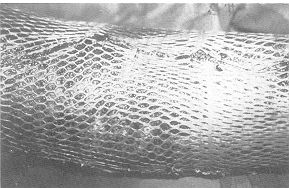
Fig. 2 -
Biobrane removed 7 days post-excision. Bed ready for autograft. |
 |
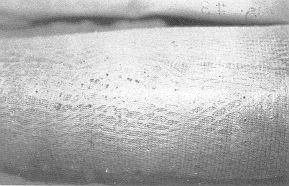 |
| Fig. 3 -
Bed grafted with a 3:1 mesh graft. |
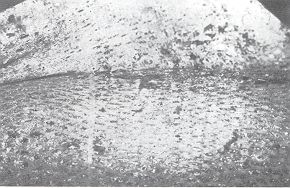
Fig. 4 -
Mesh graft covered with Biobrane. |
 |
 |
| Fig. 5 -
Seven days after grafting. Mesh closing beneath Biobrane. |
Fig. 6 -
Ten days after grafting. Biobrane removed and graft take achieved. Whole mesh closed. |
|
Case 2
This was another 14-year-old Caucasian
boy, with 45% TBSA deep bums in the face, neck, thorax and upper extremities. He underwent
surgical excision on day 4 postburn. A very deep bum on the anterior thorax induced us to
perform a fascial excision. The patient's poor general condition obliged us to use a TSS.
In this case we used a BSS (Biobrane) because of a temporary shortage in the skin bank. We
covered Biobrane with Furacin and a cornpressive dressing in order to achieve haemostasis.
The dressing was changed every two or three days. On day 11 post-burn we removed Biobrane
and found a good autograft bed. No infection was present.
Results
The use of Biobrane after early burn
wound sequential excision (Case 1) was satisfactory, because it enabled us to delay
autografting until we were sure of good conditions in the wound bed. We also noticed that
some areas of uncertain viability at the end of the first procedure became viable
recipients with no further excision. We used one sheet of Biobrane on the leg and two
sheets on the thigh and thorax.
Biobrane proved to be a good dressing over the meshed autografts. It reduced the healing
time with the mesh and the taking time of the autograft. Ten days after grafting the mesh
had closed and the graft had taken and was stable. It improved the quality, stability and
amount of graft take. We did not make any change of Biobrane.
The donor site beneath Biobrane healed in ten days and the new epithelium was of good
quality. We controlled the evolution of healing every day we made an inspection. We did
not need any change of dressing (BSS).
We were able to bath the patients whenever necessary. In Case 2, Biobrane enabled us to
delay grafting until the general state of the patient had improved. This did not cause any
deterioration of the local status of the wound.
Discussion
The adherence of Biobrane reduces the
incidence of endogenous infection, protects against exogenous bacteria, diminishes pain
and allows bathing of the patient. Adherence is slightly less than that of allografts
before day five, but after a further 72 hours it is greater.' Woodroof found practically
the same bacterial presence beneath Biobrane as beneath allografts (less than 101
bacteria/3.75 CM2).
Biobrane prevents wound dehydration, facilitates drainage of excess fluid and reduces
evaporative water loss. Evaporation beneath it is slightly more than that of skin, and
still better after day 5. Biobrane favours permeability to antibiotics.
Biobrane improves re-epithelialization :7,8 only one application is necessary, there is no
need of changes and there is no tissue aggression due to repeated changes. It is capable
of diminishing fibroblast capacity for wound contraction, maintaining the wound at up to
70% of its original size on day 21. After that it loses its efficacy.
The single application reduces pain and costs. It adapts to any body surface.
Epithelialization is visible beneath Biobrane. There is less pain when moving the joints.
It improves debridement and the patients' comfort.
The drawbacks of Biobrane are: no haemostasis, high cost, less uniformity, potential
antigenicity, risk of unusual infection or contaminants, possible hypersensitivity, and
overuse due to familiarity or negligence.
Biobrane has been evaluated for use on excised wounds.' It resulted in good beds to accept
autografts and its efficacy was comparable to that of allografts. When used to cover a
meshed autograft, Biobrane improved the take of the graft, with a substantial difference
between covered and uncovered areas. Its use over the mesh also kept the granulation
tissue within good limits and assisted epithelialization, which was improved. When used to
cover autograft donor sites, Biobrane has also been used effectively, but the healing time
and high cost do not recommend this use. We find occlusive hydrocolloids better than TSS
for managing donor sites. In conclusion, Biobrane has been shown to be an effective skin
substitute for use on excised burn wounds and over meshed autografts, and it exhibits
nearly all the ideal properties of a skin substitute. It is a substitute for allografts
when these are not available.
RESUME. Les
auteurs ont considéré l'emploi d'un succédané cutané provisoire (Biobrane) dans le
traitement des brûlures excisées (brûlures profondes). Ils ont aussi utilisé le
Biobrane pour couvrir l'autogreffe à mailles. Ils montrent que ce succédané cutané
diminue les temps de guérison et de fermeture de la greffe à mailles et améliore la
prise de la greffe. Ils considèrent aussi les sites donneurs de l'autogreffe.
BIBLIOGRAPHY
Koller J., PanAkovd P., Siska
1. et al.: The use of banked skin in excisional treatment of burns. In: "Progress in
burn-injury treatment" (Eds. Boecks W., Moserovd J.), Acco, Leuven, pp. 94-7, 1990.
Nicholas E., O'Connor M.D.,
Gallico G., Compton C.: Long-term results in major pediatric burn patients treated with
cultured skin. In: "Abstracts book of the IV European Burns Congress",
Barcelona, p. 78, 1991.
Compton C.: Cultured epithelial
autografts from seven days to seven years postgrafting. In: "Abstracts book of the IV
European Bums Congress", Barcelona, p. 79, 1991.
Hansbrough J.F.: Biologic
dressings. In: "The art and science of burn care" (Ed. Boswick J. A.), Aspen
Publications, Rockville, p. 60,1987.
Herman W.J., Wertheym E., Shafir
R.: Synthetic skin substitute for superficial paediatric burns. Arm. Medit. Burns Club, 6:
105-8, 1993.
Coenen LM.F.H., Jonkinan M.F.,
Klasen H.J. et al.: A new concept on artificial skin: the triple-layer. In:
"Abstracts book of the IV European Bums Congress", Barcelona, p. 132, 1991.
Woodroof E.A.: BiobraneR: a new
biosynthetic skin substitute. In: "Care of the bum wound" (Eds. May S.R., Dogo
G.), Karger, Basel, pp. 218-30, 1983.
Guilbaud L: Inerpan. French
multicentric study of the temporary skin substitute. In: "Progress in burn-injury
treatment" (Eds. Boecks W., MoscrovA J.), Acco, Leuven, p. 120-7, 1990.
Terr6n L, Serna C., Tejerina A.
et al.: A comparative study of three new occlusive dressings for healing of graft donor
sites versus conventional therapy. Eur. J. Plast. Surg., 16: 98-103, 1993.
E.B.A.
SCIENTIFIC PRIZE 1995
To stimulate research into the treatment of
burns, a Solvay Pharma Scientific award was presented during the E.B.A. Conference in
Verona, Italy on September 14th, 1995.
The award was presented to Dr Mamta Shah of Manchester by the President of the
European Bums Association (E.B.A.), Prof. L. Donati of Milan. Dr Marnta Shah received the
prize, which consists of a sum of money of DFL 15,000 and a certificate produced by an
artist for her work on the reduction of cutaneous scarTing by modulation of the Growth
Factor Profile.
For further information on the prize or detailed
regulations please contact the secretary of the jury:
Dr P.F. Salden
Solvay Pharma
C.J. van Houtenlaan 36
13 81 CP Weesp
The Netherlands
Tel.: +31 (0)294.477303 - Fax: +31 (0)294.417864 |
|