| Ann. Medit. Burns Club - vol. VIII - n. 3 - September 1995
REDUCTION OF BLOOD LOSS DURING PRIMARY
TANGENTIAL EXCISION WITH EPINEPHRINE INFILTRATION
Br& A.
University Medical Centre,
Department of Plastic Surgery and Burns, Zaloska, Ljubljana, Republic of Slovenia
SUMMARY. One
of the problems in primary tangential excision of bum wounds is bleeding. To reduce
bleeding epinephrine solution (2 mg epinephrine active substance in 1000 ml normal
saline) has been used to infiltrate the excision area, also using a tourniquet on the
extremities. As the amount of blood loss during the operation is not known precisely the
amount of blood transfused was recorded in order to maintain haemoglobin at 10- 12 g%.
In this study I I children and 24 adults with deep dermal and full-thickness bums
covering 10-60% body surface were randomly included. In the children the total
amount of blood given was 57.4 rut per 1% excision (one half during and one half
after the operation). In the adults the value was 142.4 ml (80.2 rut during
and 62.2 after the operation). Compared to a previous study carried out by the
author, and despite the considerable differences between patients, the results were
satisfactory, especially in the children. The main advantages of this method are the
reduction of blood loss, the prevention of uncontrollable profuse bleeding and the
slowing-down of the transfusion rate during the operation.
Introduction
Extensive and rapid blood loss during
and after primary tangential excision (PTE) of burn wounds is a serious problem and may
quickly reach extremely high values.
Since 1966, when the author started using PTE' in the first five days post-burn,
tourniquets have been used on extremities to reduce blood loss.' In other body areas there
has been no effective way of preventing bleeding during PTE except topical application of
epinephrine compresses on already excised areas and electrocoagulation of the larger
capillaries. The objective of this study was to reduce the profuse bleeding in the course
of PTE in body areas where tourniquets were not used, with infiltration of epinephrine
solution in the operative field.
The amount of blood transfusion given during the operation and on the next day was
recorded and related to one percent of excised surface. Haemoglobin values were between 10
and 12 g%.
It is very difficult to compare values of blood loss and blood transfusion in different
patients with different surgeons, different surgical techniques and possibly misleading
statistical data. A number of studies describe the problems with early excision and blood
loss. Topical epinephrine has been used by a number of authors to control excessive
bleeding. Significant haemodynamic effects of epinephrine were noted by one author."
Other authors reported no ill effects" and a detailed pathophysiological explanation
was given.
Materials and methods
After the treatment of burn shock with
crystalloids, colloids and sometimes blood, PTE was performed on day 3-5 post-burn. The
technique of excision was preferably tangential, and rarely fascial. According to the
burned area, tourniquets were used on extremities and infiltration with epinephrine
solution in other regions, and in children even in donor areas (head).
The excision started after 10 minutes and it was evident that the profuse capillary
bleeding was much reduced. The appearance and colour of the injected tissue was similar to
that under tourniquet. The bluish zone of stasis had to be removed by gradually slicing
until the "pale yellowish colour of the tissue and the moisture of the excised
surface indicated the viability of the tissue.
Body areas (for example, right upper chest, left upper chest) were injected, excised,
electrocoagulated and covered with grafts, and the following area was operated on in the
same manner.
According to our strategy, large donor areas were used to cover as much as possible with
autografts (meshed 1: 1.5 or L3). In extensive necrectomies large sheets of homografts
were also used in combination with autografts.
All operative procedures were carried out under general anaesthesia.For transfusion,
mostly packed red cells were used, and then whole blood and platelet-rich plasma if
necessary. The values of packed red cells were converted to whole blood by multiplying by
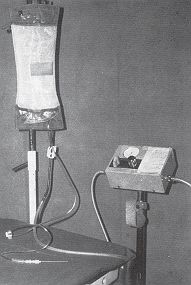
1.6.The infiltration of epinephrine solutioon was performed either by a syringue or by a
simple device using pressure from an inflatable tourniquet (Fig. 1).
|
Fig. I - A
simple device to facilitate the infiltration of epinephrine solution using pressure of the
inflatable tourniquet. |
|
The infusion set is connected to a bag
with epinephrine solution which is compressed with an inflatable tourniquet. The pressure
is set to 300 nan Hg which is enough to infiltrate the area with a needle. To stop the
flow it is necessary to compress the rubber part near the needle.
Selection of patients
The study included children and adults
randomly selected with burns covering 10-60% of body surface area (B SA), i.e. 11 children
aged 1 to 11 years (mean 4.6 ± 1. 1) and 24 adults aged 17 to 70 years (mean 34.6 ±
3.1). The excised area in one single operation was 6-28% 13SA (mean 18.0 ± 2.3) and 4-40%
13SA (mean 19.6 ± 0.5) respectively (Table 1).
Selection of vasoconstrictive solution
| |
No. of
patients |
Age |
Excised
area |
| Children |
11 |
1-11 years |
6-28% |
| |
|
mean 4.6 ± 1,1 |
mean 18 + 2.3% |
| Adults |
24 |
17-70 years |
4-40% |
| |
|
mean 34.6 ± 3.1 |
mean 19.6 ± 0.5% |
|
| Table I - Burns 10-60% BSA. Number of Patients, age and
excised area in one operation |
|
M1 of blood
given for 1%
excision |
|
Children (No 11) |
Adults (No 24) |
During the operation |
29.2 ± 6.7 mi |
80.2 ± 2.5 nil |
After the operation |
28.2 ± 6.1 ml |
62.2 2.2 ml |
| |
57.4 mI |
142.4 rat |
Next day |
7.5 ± 4.0 rat |
33.6 ± 3.4 nil |
|
| Table 2 - Burns 10-60% BSA. blood transfusion given for 1%
excised necrosis during the operation, after and next day |
|
Blood transfusion
in %
of blood volume |
0-24% |
For early
excision in %
of body surface |
3-15% No. 8 |
25-49% |
10-25% No. 5 |
50-74% |
10-33% No. 6 |
75-99% |
20-38% No. 4 |
100-143% |
18-35% No. 7 |
Blood
transfusion during the operation and after on the same day in order to maintain the Hb
values between 10-12 g%. In the group 30 children, aged 3 months-14 years with burns
10-60% BSA. the amount of transfusion was calculated in the percentage of respective blood
volume. Less than 1/4 of blood volume was needed in the grooup of 8 children where the
necrotic tissue excision was 3-15% BSA. On the other hand in the group of other patients
where 18-35% excision was performed more than the whole blood volume was Deeded to keep
the Hb level between 10- 1 2g%. |
|
| Table 3 - Bums 10-60% BSA., early excision 3-4 days P.B.,
children 3 months to 14 years, No. 30 |
|
Epinephrine HCl solution containing 2.0 mg
epinephrine active substance in 1000 ml of normal saline in the amount of 20 nil per 100
crn' was injected subcutaneously. The total amount of injected solution varied from 100
ral in limited excisions to 500 or 1000 mI, in extensive excisions.
Results
In children the amount of blood given
for each 1 percent of the body surface debrided of eschar was 29.2 ± 6.7 mI during the
operation plus 28.2 ± 6.1 ral after the operation on the same day. The total amount was
57.4 ml ranging from 116 ml for 22% excision to zero for a 6% excision. On the next day
additional transfusion of 7.5 ± 4.0 ml per 1 % excised eschar was sometimes needed.
In adults the amount of blood given for excision of 1% BSA. was 80.2 ± 2.5 ml during the
operation plus 62.2 ± 2.2 ml after the operation on the same day. The total amount was
142.4 ml, ranging from 344 ml for a 12.5% excision including the face to zero for a 12%
excision on the chest. On the next day additional transfusion of 33.6 ± 3.4 ml for 1% of
excised tissue was sometimes needed (Table 2).
Discussion
There are two problems in bum surgery:
estimation of bum depth before and during the operation and estimation of blood loss.In
PTE, which is carried out during the first few days post-burn, the patient is often
haemodynamically unstable with a low platelet count.The blood transfusion during the
operation has to cover the blood loss not only in excised areas but also in donor areas.
In my first study' in 1988 1 measured the blood transfusion during PTE in 30 children aged
from 3 months to 14 years with a percentage of excised bum eschar in one operation of
3-35%. All bums were greaFer than 10%. The given blood transfusion was expressed as a
percentage of circulating blood volume" and varied according to the percentage of
excised burn surface (Table 3).The conclusion was that in extensive PTE significant
amounts of blood transfusion were necessary and we therefore started looking for ways of
reducing it.In the present study epinephrine solution was injected in all areas where a
tourniquet cannot be used and in children also in donor areas. After the injection of
epinephrine solution, vasoconstriction is evident after a few minutes and bleeding after
tangential excision, which is carried out after ten minutes, is minimal. It is therefore
much easier to electrocoagulate larger capillaries which are otherwise submerged in
profuse bleeding.
In PTE, in the first three days, oedema fluid is still present. This facilitates the
excision but probably reduces the action of adrenaline which is diluted and washed out.
Before the action of adrenaline terminates, which occurs in approximately 20 minutes, it
is necessary to electrocoagulate larger capillaries, cover the area with grafts
(preferably mesh grafts are used) and apply compressive dressings. It is possible to
overlook persistent bleeding of some capillaries, which necessitates post-operative
coagulation.
In our series approximately half the blood was given during the operation and the other
half post-operatively. On the next day small amounts were occasionally necessary.
Large differences were noted among the patients for blood replacement. In children the
range was from 116 ml per 1% excised necrosis in a 22% excision to 0 ml for a 6% excision.
In adults differences were larger and ranged from 344 ml per 1 % in a 12.5 % excision
including the face to 0 ml for a 12% excision in other regions. The side-effects of
epinephrine in extensive bums are insignificant because of "down regulation and
alteration in affinity of beta receptors. In our patients a transitory rise of blood
presssure and/or pulse rate was noted which returned to normal when the action of
adrenaline terminated.
Conclusion
The use of adrenaline solution is a
simple and effective aid in PTE which controls profuse capillary bleeding. In extensive
burns the adverse effects are minimal and transitory.
RESUME. L'hémorragie
constitue un des problèmes de l'excision tangentielle primaire des brûlures. Pour la
réduire, une solution d'épinéphrine (2 mg d'épinéphrine substance active dans
1000 ml de solution saline normale) a été utilisée pour infiltrer la zone d'excision,
avec en plus un tourniquet dans les extrémités. Puisqu'il est difficile de savoir avec
précision la quantité de sang perdu pendant l'opération chirurgicale, l'auteur de cette
étude a noté la quantité de sang transfusé pour maintenir l'hémoglobine à 10-12 g%.
L'étude randomisée comprenait 11 enfants et 24 adultes atteints de brûlures
dermiques profondes et à toute épaisseur dans 10-60% de la surface
corporelle. Chez les enfants la quantité totale de sang administré était 57,4 ml
pour 1% d'excision (moitié pendant et moitié après l'opération). Chez les adultes la
quantité était 142,4 ml (80,2 ml pendant et 62,2 ml après
l'opération). Par rapport à une étude précédente du même auteur, et malgré
les grandes différences entre les patients, les résultats ont été satisfaisants,
particulièrement pour ce qui concerne les enfants. Les avantages principaux de cette
méthode sont les suivants: réduction de la perte de sang, prévention de l'hémorragie
abondante et incontrollable, ralentissement de la vélocité de transfusion pendant
l'opération.
BIBLIOGRAPHY
- Br66 A., Zdravi6 F.: Lessons learnt from 2409 bum
patients operated by early excision. Scand. J. Plast. Surg., 13: 107-9, 1979.
- Br6i6 A.: Primary tangential excision for hand bums.
In: "Hand clinics" (Ed. Grossman J.), Vol. 6, No. 2, p. 211-9, Saunders,
Philadelphia, 1990.
- Spijker R.E.: Anaesthesia for early excision of
extensive full-thickness bums. Symposium for the treatment of burns, Prague, Abstracts p.
55-7, 1973..
- Snelling C.: Quantitative evaluation of blood loss
during debridement and grafting of bums. Cand. J. Surg., 25: 416-7, 1982.
- Kcaley G.P., Shafer B., Lewis P.W. et al.:
Post-operative time course of coagulation factors in bum patients. Proceedings of the ABA
23rd Annual Meeting. Abstracts book, p. 105, 1991.
- Budny P.G., Regan P.J., Roberts H.N.: The estimation
of blood loss during burns surgery. Burns, 19: 134-7, 1993.
- Timonen R.M., Pavlin E.G., Hasche R.H. et al.:
Epinephrine levels pre- and post-application of topical epinephrine during bum
surgery.Anaesthesia, 57 (suppl.): A 138, 1982.
- Snelling C., Shaw K.: The effect of topical
epinephrine hydrocloride in saline on blood loss following tangential excision of burn
wounds. Plast. Reconstr. Surg., 72: 830-4, 1983.
- Roberts A.: The effect of topical epinephrine on
blood loss following tangential excision of bum wounds. Plast. Reconstr. Surg., 74: 450-1,
1984.
- Stratton J., Pfeifer M,, Ritchie J. et al.:
Hemodynamic effects of epinephrine: concentration effects study in humans. J. Appl.
Physiology, 58: 1199-1206, 1985.
- Glasson D.: Topical adrenaline as a hemostatic
agent. Plast.Reconstr. Surg., 74: 451-2, 1984.
- Martyn J.A.: "Acute management of a burned
patient", pp. 191-3, Saunders, Philadelphia, 1990.
- Janzekovic Z. In: "Present clinical aspects of
bums: a symposium", (Ed. Derganc M.), pp. 99-215, Maribor, 1968.
- Nadler S.B., Hildago J.U., Bloch T.: Prediction of
blood volume in normal human adults. Surgery, 51: 224, 1962.
MBC - PREVENTION
CAMPAIGN
The MBC, in the context of the activities laid down
in its Statute and intended to promote burn prevention campaigns, has produced the
following videotapes:
The Prevention of Bums in Children
The Prevention of Electrical Bums in Everyday Life
The Prevention of Electrical Bums at Work
The Prevention of Industrial Disasters
How to Defend ourselves from Fire
How to Defend ourselves from Forest Fire
The tapes have been dubbed in English, French,
Arabic, Italian, Spanish, Greek and Turkish and come in two versions, U-MATIC and VHS.
All the tapes are available entirely free of charge to MBC Members who apply in writing to
receive them explaining their reasons and undertaking to use them exclusively to promote a
bum prevention campaign in their respective countries.
For non-members of MBC the tapes are available at a cost of US$ 25 each, including postal
charges.
Please address requests to: Annals of Burns and Fire Disasters, Divisione di Chirurgia
Plastica e Terapia delle Ustioni, Ospedale Civico, Via C. Lazzaro, 90127 Palermo, Italy.
Tel.: 39.91.6663631 Fax: +39.91.596404. |
|