| Ann. Medit. Burns Club - vol. VIII - n. 3 - September 1995
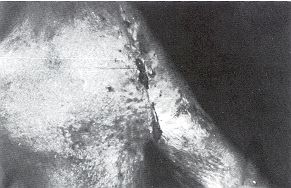
ISLAND PARASCAPULAR FLAP FOR THE TREATMENT OF DIFFUSE AXILLARY BURN SCAR CONTRACTURE Shalaby H.A. Plastic Surgery Unit, Tanta University Hospitals, Tanta, Egypt SUMMARY. Fifteen parascapular flaps based on the oblique branch of the circumflex scapular artery were used to correct post-burn axillary contractures in 12 patients. The contractures were of the diffuse type (type IV), in which scarring involves all the anterior and posterior axillary folds, usually in association with the hair-bearing area. All the flaps remained totally viable and were successfully used to release the contractures. The donor area was either closed primarily or covered by split-skin graft. Introduction Burns around the axillary region frequently lead to contractures which may be diffuse' and severe (Fig. 1). Hanumadass et al.' classified post-burn axillary contractures in four types according to the local anatomic conditions. The diffuse type (type IV) is characterized by involvement of the hair-bearing area, the anterior and posterior axillary folds, and the periaxillary region. In their view the procedure of choice is a single incisional release and splitskin grafting. A tie-over bolus, a bulky dressing and a plaster of Paris splint are applied. There is usually good take of the graft, as part at least is laid over muscles. However, unless the arm is kept in abduction for at least 3-6 months',' with a cumbersome splint, some degree of recurrence of contracture is inevitable and a repeat proce~ dure is often required. If the graft does not take, a prolonged and often frustrating period ensues.
To overcome the problem of recurrence, several alternative techniques have been proposed. These include the inner arm fasciocutaneous flap,' the scapular island flap,' the fasciocutaneous flap from the anterolateral or posterolateral aspects of the chest,' the parascapular flap,' and the free flap. In a previous study,' we reported our evaluation of different techniques used in the treatment of post-burn axillary contractures. For the diffuse type the procedure of choice was the transverse scapular flap. Since then, i.e. 1990, we have shifted to the parascapular flap, and this study is an evaluation of this kind of flap, with a retrospective comparison to the transverse scapular flap. Technique The flap is designed while the patient is standing up, with the anus adducted to the sides. The circumflex scapu~ lar artery passes through the triangular space between teres major, teres minor and the long head of triceps.' The cutaneous branch passes through the deep fascia on the lateral border of the scapula, 2 cm above and medial to the apex of the posterior fold of the axilla. When the posterior axillary fold is distorted by scarring, the site of the cutaneous branch can be defined by drawing a point mirror-image to the contralateral side. The oblique branch passes downwards and medially, parallel to the lateral border of the scapula. The long axis of the flap is therefore drawn along the lateral border of the scapula. The flap can be extended down to the lower border of the last rib. After release of the axillary contracture, the defect is measured and a suitable flap designed with its base at the site of the perforator. If the defect is more than 10 cm, the flap can be used to cover the central area with grafting above and below it. The flap is raised, starting from below. The deep fascia overlying the latissimus is included in the flap and when it is dissected free from the muscle a rich vascular network can be seen on the underside of the fascia. When the teres major muscle is reached, its media] border is followed up to the pedicle vessels. At this stage, the pedicle vessels are mobilized from the triangular space. The medial and lateral incisions are then completed and the flap is either left pedicled or transformed into an island. If scarring at the donor area is extensive, it is better to leave it pedicled. The flap is transposed to lie in the axillary defect and sutured in place. When the defect is larger than the flap, split-skin graft is applied above and below the flap.Extensive undermining is needed to close the defect if it is more than 8 cm wide. As there are often other skin grafts and scars in the vicinity, a split-skin graft to close the donor defect is an acceptable and safe procedure.A tie-over dressing is applied to the grafted areas, and a light dressing is applied over the flap. The arm is kept in abduction for 1-2 weeks post-operatively, until the sutures are removed. Prophylactic antibiotics are given for 3-5 days. The first dressing is done on the seventh post-operative day. Follow-up visits and physical therapy for the shoulder start in the third week. Results The parascapular flap was used to
reconstruct 15 axillae in 12 patients (7 females and 5 males, age range from 4 to 52 years
with a mean of 23 years) (Table 1). The contracture was on the right side in four
patients, on the left side in five, and bilateral in three.
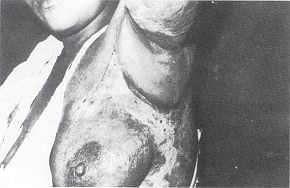
The flap was thin and defined the concavity of the axilla in 12 axillae. In two rather obese patients the bulkiness of the flap was noticeable bilaterally in one patient and on the left side in the other (Fig. 4). The average hospital stay was 7-15 days, with a mean of 9 days. The maximum follow-up was 2.5 years. Discussion The scapular flap, based on the
transverse cutaneous branch of the circumflax scapular artery, was first described by dos
Santos' following 70 cadaver dissections. In 1982, Nassif et al.11 described the
parascapular flap and used it as a free flap. The circumflex scapular arter y passes
through the triangular space, courses around the lateral border of the scapula and directs
itself towards the cutaneous territory of the back. A vascular pedicle at least 6 cm long
can be dissected, which makes the flap ideal as an island to the axilla. The artery and
accompanying veins are constant and of large size, averaging between 2 and 3 min in
diameter. The dissection of the flap is easy and it can be raised within 30 minutes. The
deep fascia overlying the latissimus dorsi must be included in the flap. When it has been
dissected free from the latissimus, the medial border of teres major has to be followed
upwards as far as the vascular pedicle of the flap. Once the vascular pedicle is
mobilized, the remaining dissection is easy and it can be transposed as pedicle or island.
When transposed as pedicled, the dog-ear is minimal as the angle of rotation is acute. The
pedicled flap is therefore preferable, especially in scarred donor areas. RESUME. L'auteur décrit l'emploi de 15 lambeaux parascapulaires basés sur l'artère scapulaire circonflexe utilisés pour corriger des rétractions axillaires dues aux brûlures dans 12 patients. Ces rétractions étaient du type diffus (type IV), dans lequel la cicatrisation touche tous les plis axillaires antérieurs et postérieurs, normalement en association avec la zone pileuse. Tous les lambeaux sont restés complètement viables et ont été utilisés avec succès pour libérer les rétractions. Le site donneur a été ou fermé primairement ou couvert avec une greffe cutanée d'épaisseune variable. BIBLIOGRAPHY
|