| Ann. Medit. Burns Club - vol. VIII - n. 3 -
September 1995
PREVENTION OF THERMAL AND CHEMICAL INJURIES
Puls M.,
Kónigová R., Bohm T., Mládek D.
Center of Burn Medicine, 3rd Medical Faculty, Charles University, Prague, Czech Republic SUMMARY. Burn injuries lead to permanent changes in the medical condition and lifestyle of many patients. This article reminds us of the fundamental differences in the causes of these injuries in the two major groups of patients, defined by NovA (1986) as children and adults. Based on the evidence and the conditions of 421 hospitalized patients subdivided into three age groups (0-3 years, 3-15 years, adults), concrete statistic information is provided on the percentage frequency of the injuries, and the cause of each injury is defined. It is concluded that in children these injuries are due to their varied interests, after-school activities, inexperience, recklessness and the lack of parental (or other) supervision. The degree of the bums becomes more severe, leading to the fatal outcome that could have been prevented. Introduction Every year more and more persons become casualty cases, as a result of the increase in various types of industrial production, the mechanization of agriculture, new forms of transport, more widespread sports activities, and terrorist incidents. Injury is defined as a sudden event, violent in nature, in a limited time, out of the victim's control, and with immediate short- or long-term consequences. The first step in the prevention of serious bum injuries is the prevention of their occurrence - a concept that is valid for all age groups. This is however a very complicated problem from the technical and organizationallbeha~ vioural point of view. On the basis of the information we have gathered, we suggest that education and prevention should begin in the home and continue at school and then at work and among the general public. The major role in education is played by parents, followed by primary and secondary school teachers, work-place supervisors and inspectors, technicians, construction designers and workers, as well as psychologists and physicians. The experience of surgeons and psychologists, with their wide knowledge of cases treated in bum medicine, is also valuable in the prevention of bums. One of the oldest and most complex methods of classifying burn cases is the NovAk system, according to which cases are classified in six groups on the basis of the cause of injury: industrial, domestic, transport, sport, agricultural and criminal. Thermal and chemical injuries most often occur in the industrial, domestic and transport categories. Global statistics show that burn injuries in children most often result from a lack of parental supervision. The parent may not be familiar with, or may underestimate, the potential danger of a situation where injuries frequently occur. The general public are often uninformed about the various possibilities and ways of sustaining burn injury and are also frequently ignorant of the methods and principles of first aid care. The treatment of bums and thermal and chemical injuries is achieved at great expense, requiring the most modern medical equipment and the co-operation of various medical disciplines. For these reasons stress must be placed on the importance of the prevention of these injuries, which can have a tragic outcome not only for the patients and their family but also for society at large. Apart from the functional and aesthetic aspects, various psychological and internal complications develop which impede the patients' return to a normal lifestyle at school or at work, or in their search for a partner. Materials and methods In this retrospective
study we attempt to determine the most common mechanisms of burn injuries in the years
1990 and 1991 for each of the individual age groups. We began with the assumption that the
major causes of the injuries are: Results In the year 1990,
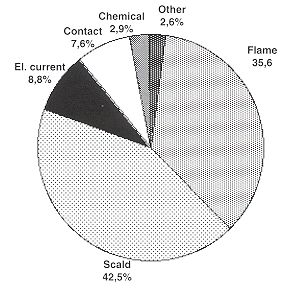
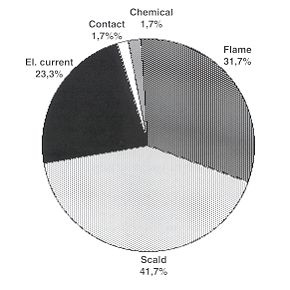
421 patients were registered with burn injuries (Fig. 1).
As said,
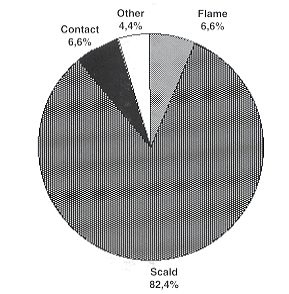
the major cause of injury was scalding, which alone caused 82.4% of burns (89.5% caused by
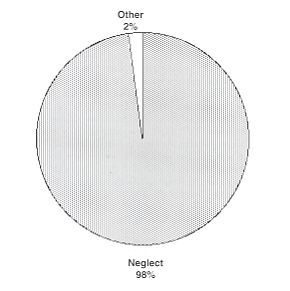
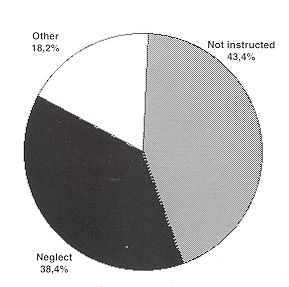
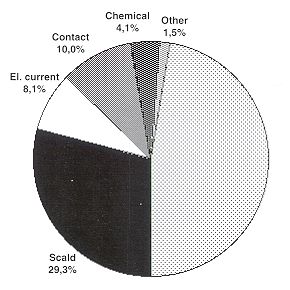
spilling, 10.5% by su · lack of parental
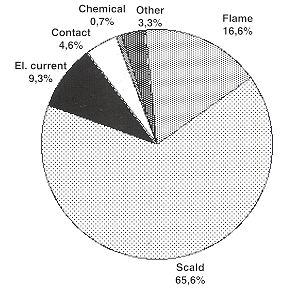
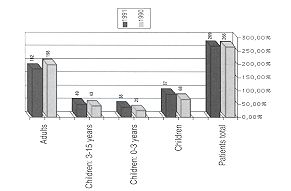
(or other) supervision (98%) The information concerning patients in the 3-15 years age group is shown in Fig. 5. In this age group, we found a larger variety of mechanisms for burn injuries, resulting from increased activity (Fig. 6). We also found that in this age group a larger percentage of the injuries was caused by handling benzene or other flammable liquids, which contributed to 42.9% of open-flame burns and 13.3% to the total bums within this age group. We also attempted to record cases which arose from the use of synthetic fibres and material. Fig. 7 shows the mechanisms of injury in the group of adults in the year 1990. Our final purpose was to compare the various cases which occurred in a ten-month period in 1991 and a corresponding tenmonth period in 1990. This survey regarded patients hospitalized in the Prague Burn Centre and the Prague Bulovka Department of Paediatric Surgery. A comparison of the numbers of burn patients admitted and treated over the two tenmonth periods (1990 and 1991) is presented in Fig 8. There is a marked increase in bum injuries among children in the year 199 1, especially in the youngest age group.Discussion The basis for this discussion lies in the remarkable difference between the results derived from research by ISBI (19% burns by open flame, 66% by scalding) and that done by our Burn Centre (35% by open flame, 42.5% by scalding). After dismissing the possibility of an error in the home. The fact which requires emphasis, and which we repeatedly encountered in our studies, is that the situations which arise and may result in fatalities were most often a result of carelessness, forgetfulness, lack of concentration, and lack of skill and experience.
Obviously,
it is necessary to inform the public about the proper methods of prevention and treatment.
The initial task that we face is the development of an organized progamme for the
prevention of these injuries. This type of campaign must have definite methods and goals. Conclusion In the formulation of a programme
for the prevention of thermal injuries we consider the following points 300,00% important:
calculations, we were unable to find a reasonable explanation for this difference. RESUME. Les brűlures causent des changements permanents dans les conditions physiques et dans la vie des patients. Cet article nous rappelle les différences fondamentales entre les causes de ces lésions dans les deux catégories principales des patients, définies par Novŕk (1986) comme les enfants et les adultes. Sur la base de l'évidence et des conditions de 421 patients hospitalisés, subdivisés en trois groupes selon l'âge (0-3 ans, 3-15 ans, adultes), les auteurs présentent des informations statistiques concrčtes pour ce qui concerne la fréquence en pour cent des lésions, et définissent les causes. Ils concluent que chez les enfants ces lésions sont causés par leurs divers intéręts, les activités en dehors de l'école, l'inexpérience, l'insouciance, et le manque de surveillance des parents ou d'autres personnes. Le degré des brűlures devient plus sévčre, avec des conséquences fatales qui auraient pu ętre évité BIBLIOGRAPHY
|