| Ann. Medit. Burns Club - vol. VIII - n. 3 - September 1995
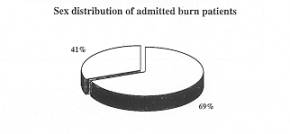
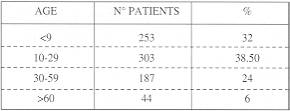
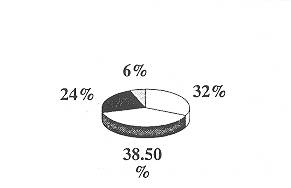
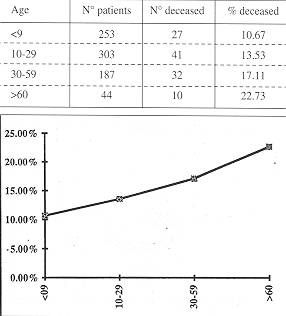
COST/BENEFIT VALUE OF A BURN UNIT AT THE AMERICAN UNIVERSITY OF BEIRUT MEDICAL CENTER Atiyeh B.S., Saba M. American University of Beirut Medical Center, Beirut, Lebanon SUMMARY. In order to assess the value of establishing a burn unit at the American University of Beirut Medical Center, a retrospective study was conducted on all burn patients admitted to the Centre between 1975 and 1993. All patients were entered into the hospital computer system following the ninth Revision of the International Classification of diseases. A total of 787 patients were computed, with an overall mortality rate of 13.98%. An average of 40 to 45 burn patients were admitted to the hospital each year, constituting about 0.25% of all hospital admissions and 1% of all surgical admissions. Distribution of the burns by age, sex, involvement of specific anatomic sites and extent was evaluated. Despite the fact that these patients were treated in a regular surgical ward, the final outcome was not worse than that reported from major burns centres. This raised the question of the wisdom of establishing a small burn unit in a private institution with tight budgetary restrictions. It may be economically much wiser in small countries like Lebanon to establish one central burn unit with the assistance of the governmental authorities instead of creating highly expensive small units. Nevertheless, the necessity of having a burn centre in a teaching institution should not be overlooked. The academic value of such a centre by far justifies the cost. Introduction In order to assess the value of establishing a small burn unit at the American University of Beirut Medical Center (AUB-MC), a retrospective study was conducted on all burn patients admitted to our centre between 1975 and 1993. Any feasibility study for the establishment of a burn unit should start by estimating the needs of the community. Unfortunately, valid national burn statistics and burn epidemiological studies are not available in Lebanon. The AUB-MC being the biggest and most prestigious medical referral centre in the country, in addition to having been the only properly functioning hospital in the western sector of the city during the long Lebanese war which corresponds to the study period, it was judged that burn patients admitted to our hospital roughly reflected the community burn status. A total of 787 burn patients were admitted for an average of 40 to 45 burn victims a year. Many more of course were treated on an ambulatory basis and many patients had to be transferred to other hospitals for lack of space, but almost all the transferable critically burned patients presenting to our emergency room were admitted. Material and methods All patients admitted to the hospital were entered into the hospital computer system following the ninth Revision of the International Classification of Diseases. As became evident, the entering data of the 787 burn patients were not accurate. Many lacked an exact estimate of the extent of the burn injury, and many more lacked an exact reference to the anatomic distribution of burns. Any detailed analysis would have necessitated the review of charts, but for the sake of the present study the data gathered were adequate to reach valid conclusions. Results Between 1975 and 1993, 787 burn patients were admitted to our hospital for an average of 40 to 45 patients a year, corresponding to 0.25% of all hospital admission and 1% of all surgical admissions. Of the bum patients admitted 59.34% were male and 40.66% female (Fig. 1). 70.65% of the patients were under 30 years of age, and 32.15% were under the age of 9 years (Fig. 2).
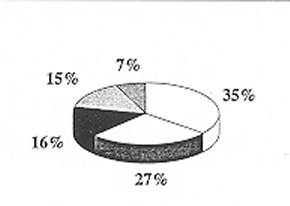
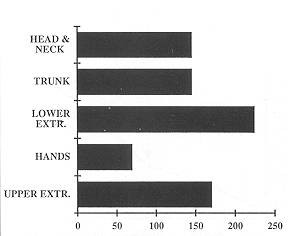
Sex distribution of admitted burn patients Thirty-eight per cent had burns in more than 50% TBSA (Fig. 3). Information about burns in specific areas of the body was available for 466 patients. 36.5% had burns in the upper extremities, 15% in the hands, 49% in the lower extremities and 315 in both the trunk and the head and neck area (Fig. 4).
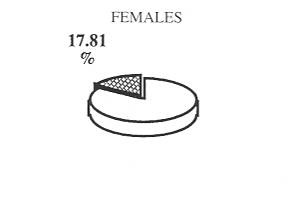
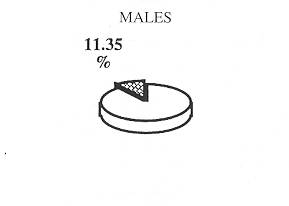
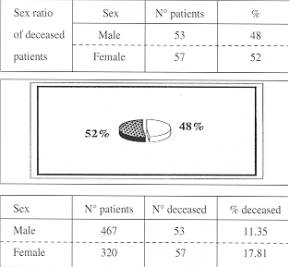
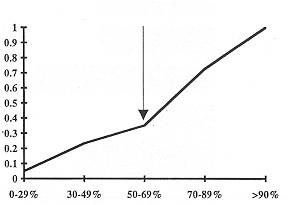
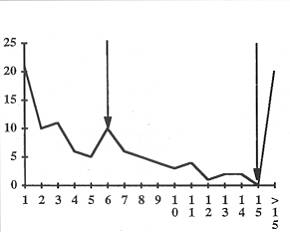
The overall mortality rate was 14%. Of the deceased patients 52% were female and 48% male. 61.5% were under 30 years of age. The relative mortality rate for males was 11 % and for females 18% (Fig. 5). The relative mortality for the various age groups ranged between I I and 23% and the mortality rate increased with age (Fig. 6). 228 patients were classified according to percentage TBSA burn. In these patients mortality rose sharply in burns of more than 70% TBSA and reached 100% in bums of more than 90% (Fig. 7). The time of death was mostly within the first week or else more than 15 days after the bum injury (Fig. 8).
Discussion The most striking feature about this analysis is the small number of burn patients admitted per year and the extremely small percentage of bum admissions compared to total hospital admissions.
This definitely does not mean that burn injuries are rare in Lebanon - it means that serious burns with life-threatening conditions could be relatively rare. In the absence of accurate statistics, it not possible to know this for certain, but as things stand now there is more demand for treatment of less critical burns than for life-threatening lesions, to judge by the large number of patients presenting to our out-patient clinic with burn contractures. Such bums are mostly attended to by a senior member of the family, a neighbour, a pharmacist and very often by a fireman in the infirmary of the local fire stations, but only rarely by a physician and hardly ever by a plastic surgeon in a major referral centre.
The majority of minor burns and sometimes
more serious burns are treated at local fire stations with a topical ointment, the
composition of which is keptjealously secret by the fire brigade. Patients are referred
late to our centre only if they fail to heal after several weeks or months of topical
treatment or because of contractures. Conclusion In conclusion, the needs for a small country like Lebanon in the field of burn management are the following:
Prevention of burns is always the best treatment. Education of the public is of extreme importance, and more important still is the education of the Lebanese population about proper bum management and where it can be delivered, so that our fire stations will cease to be the major burn treatment centres. RESUME. Pour évaluer l'utilité de créer une unité de brûlures au Centre Médical de l'Université Américaine de Beyrouth, les auteurs ont effectué une étude rétrospective de tous les patients hospitalisés dans leur centre entre 1975 et 1993. Tous les patients ont été entrés dans le système informatique de l'hôpital selon la neuvième révision de la classification internationale des maladies. En tout 787 patients ont été évalués, avec un taux de mortalité de 13,98%. En moyenne 40 à 45 patients ont été hospitalisés tous les ans, ce qui représente environ 0.25% de toutes les hospitalisations et 1 % des hospitalisations qui nécessitaient un traitement chirurgical. La distribution des brûlures selon l'âge, le sexe, la présence de lésions dans des sites anatomiques particuliers et l'étendue a été évaluée. Ces patients ont été traités dans une salle chirurgicale normale mais quand même les résultats finals n'étaient pas inférieurs aux résultats obtenus dans les grands Centres de Brûlés. Cette considération a soulevé la question de la prudence de la création d'une petite unité de brûlures chez une institution privée avec des restrictions budgétaires très serrées. Il pourrait être économiquement plus sensé dans les petits pays comme le Liban d'établir une unité de brûlures centrale avec l'assistance des autorités gouvernementales au lieu de créer plusieurs petites unités très coûteuses. Il ne faut pas néanmoins oublier la nécessité d'avoir un centre de brûlés dans un centre hospitalo-universitaire. La valeur académique d'un tel centre justifie abondamment le coût. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||