| Annals ofBurns and Fire Disasters - vol. VIII - n. A - Deceinber
1995
SENILITY AND BURNS - FOUR YEARS'
EXPERIENCE
lliopoulou E, Lochaitis A, Kalophonou
M, Kapositas E, Komninakis E, Poulikakos, L, Daniel-Seferi A.
Department of Plastic and
Reconstructive Surgery and Burn Unit, K.A.T. District Hospital, Athens, Greece
SUMMARY. In the
four-year period 1990-1994, 185 patients aged over 65 years with mixed full- and partial
-thickness burns in a mean total body surface area (TBSA) of 26.8% were admitted to our
Bum Unit. In the majority of cases the aetiology was therrial injury (11ame 63%, scalding
19%, contact 10%, friction 5%, chemical burns 3%). Over one~third of the accidents
occurred in a closed environment and were domestic. Inhalation injury was present in 23%
of the patients (mortality 100%). Overall mortality was 33% (mean age 79.7 years vs. 72.0
years in surviving patients, mean TBSA 40% vs. 23% in surviving patients). The leading
causes of death were major cardiopulmonary complications (70%), infection (18%) and
hypovolaernic shock (3%). Our results have led us to the conviction that immediate and
intensive treatment in combination with very early mobilization will lead to rapid healing
and rehabilitation in many of these eleterly patients.
Introduction
The improved quality of life and the
great progress in medical and social assistance in Greece in recent decades have led to a
considerable rise in life expectancy. This progress, together with the phenomenon of the
continuously falling birth rate, has led to a doubling of the percentage of the elderly in
the overall Greek population from 6.8% in 1951 to 13.9% in 1990.
This considerable rise in the life expectancy of the Greek population has resulted in an
increased incidence of accidents, including burns, while a variety of social and financial
problems have complicated facilities for treatment and rehabilitation.
The definition of "elderly" is generally accepted as corresponding to the age of
65 years and older. Parallel to the increase in life expectancy there has been an
increased rate of hospitalized burns among the elderly. Geriatric patients have decreased
physiological reserves and a significant number of previous pathologies, both of which
factors give rise to increased risks of complications and death following burn injury.
Materials and methods
During a four-year period (1990-1994)
185 patients aged 65 years and over were treated at K.A.T. General District Hospital Burn
Unit. This represented 17% of all burn admissions.
Age and sex
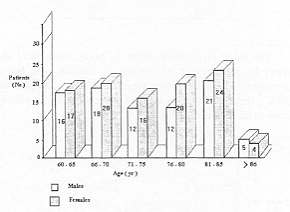
The mean age of the patients was 74.5 years (range 65-96 years). Women predominated in all
age groups (ratio 100:85), except in the over 85-year-old age group (Fig. 1).
 |
 |
| Fig. 1 -
Distribution by age and sex. |
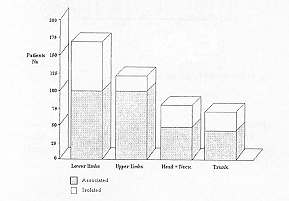
Fig. 2 - Location of burns, |
|
BURN EXTENT |
N' |
% |
0
- 30% |
139
|
75 |
31
- 60% |
28
|
15 |
61
- 100% |
18
|
10 |
|
| Table 1 - Percentage of surface area involved |
|
Depth
In terms of depth of injury most patients presented mixed partial- and full-thickness
lesions (60%). Twenty-two per cent suffered superficial partial-thickness burns and 18%
presented isolated full-thickness burns (Table II).
BURN DEPTH |
N' |
% |
Mixed
partial and full-thickness |
111 |
60 |
Superficial
partial thickness |
33 |
22 |
Full-thickness |
41 |
18 |
|
| Table
II - Depth of injury |
|
Location
The most commonly affected body parts were
the lower limbs alone (82%) or in association with burns elsewhere. The upper limbs were
affected in 107 patients (58%), the head and neck in 55 patients (33%), and the trunk in
65 patients (35%) (Fig. 2).
Aetiology and circumstances
Thermal burns were the commonest cause of injury (flame, 63%; scalding, 19%; contact, 10%,
friction, 5%; chemical bums, 3%) (Table 111). Over one-third occurred in closed
spaces and were domestic. Elderly patients who lived alone represented one-third of our
series and tended to present burns of greater extent (36% TBSA) than patients living with
their family (25% TBSA). Four patients presented flame lesions sustained in traffic
accidents, and ten presented friction injuries due to being dragged along the ground by
vehicles. Only five cases were registered as suicide attempts.
AETIOLOGY |
N' |
% |
Flame and contact |
135 |
73 |
Scalding |
35 |
19 |
Friction |
10 |
5 |
Chemicals |
5 |
3 |
|
| Table III - Burn aetiology |
|
Sociofinancial circumstances
Loneliness and low financial status (with or without social support) were common to most
patients. Only 25% of the patients enjoyed a medium/high financial status.Previous
pathology The majority of cases presented significant chronic prebum morbidity.
Cardiorespiratory and circulatory problems predominated among the patients who died (Table
IV).
| PREVIOUSE
PATHOLOGY |
SURVIVAL |
DEATH |
TOTAL |
Hypertension |
19 |
13 |
32 |
Circulatory
insufficiency |
15 |
9 |
24 |
Diabetes |
15 |
10 |
25 |
Respiratory
insufficiency |
10 |
5 |
15 |
Psychiatric
problems |
12 |
3 |
15 |
Alcoholism |
10 |
6 |
16 |
Coronary
insufficiency |
8 |
1 |
9 |
Neuropathology |
4 |
3 |
7 |
|
Table IV - Previous
pathology and the correlation between survival and death |
|
Concomitant pathology
Only ten patients presented concomitant lesions (fractures in seven cases, craniocerebral
contusion in three cases).
Delay in admission
One hundred and fifty-four patients were admitted 28 hours after the accident and 21 after
2-10 days, following transportation from other hospitals or regions at some distance from
Athens. This delay influenced overall mortality.
Hospitalization
The mean hospitalization period was 15 days (range 090 days).
Treatment
The patients were treated uniformly. Antishock resuscitation formulae based on the
Parkland method were the rule in the majority of patients, together with close attention
to vital parameters, previous pathology, and the development of complications. Intubation
was performed in patients suffering from inhalation injury. None of these survived.
Low molecular heparin (Fraxiparine, Clexane) was started as a preventive measure in the
first hours post~burn. Antibiotics were used in relation to concomitant illnesses. Early
excision and skin grafting were performed in 38% of the patients (TBSA 1-30%). In five
cases amputation of the lower or upper limbs was the elective treatment, owing to the
severity of the burn lesions (deep burns involving fat, muscle, or bone.) Early
kinesiotherapy and respiratory gymnastics were initiated 2-4 days post-burn (when patients
were haemodynamically stable). Nutritional management was intensive, with enteral
administration as the mode of choice.
Complications
The majority of our patients suffered at least one complication due to previous pathology,
the post-burn condition, or failure of treatment.
Mortality
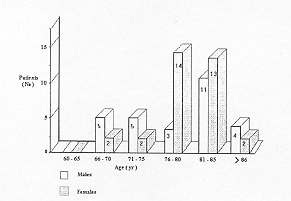
The overall mortality rate was 33% (61 deaths). The mean age of the deceased was 79.7
years vs. 72.0 years for those who survived (Fig. 3). Although females were
predominant in all age groups, there was higher mortality in younger men (60-75 years). In
the over 75-year-old age group, this proportion was inverted.
 |
 |
| Fig. 3 -
Mortality distribution by age and sex. |
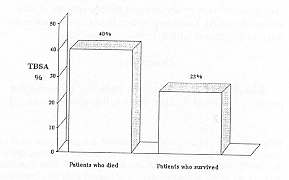
Fig. 4 - Correlation
between TBSA and mortality. |
|
The mean burn extent among the patients
who died was 40% TBSA versus 23% TBSA among the survivors (Fig. 4). The majority of
the deceased had full-thickness burns (56%). Face burns, when associated with inhalatory
injury, were fatal. Previous pathology played an impportant role in the course of the burn
disease. All the deceased patients presented at least one previous pathological condition.
Concomitant pathology also greatly influenced the outcome, ten cases (fractures,
craniocerebral lesions) having a fatal outcome.
Discussion
Our series of 185 cases represents 17%
of all our bum admissions over a four-year period (1990-1994). In line with the
demographic characteristics of the Greek population there was a prevalence of female
patients (female/male ratio: 100:85).
Most patients (75%) presented a burn extent of 1-30% TBSA, and most patients (60%)
suffered mixed partialand full-thickness lesions. The body region most frequently burned
was the lower limbs alone or in association with other regions. Lower extremity burns,
requiring longer decubitus, were associated with increased mortality, due to diminished
speed of reaction and of life support reflexes in general. In addition, these patients
frequently presented a greater number of previous diseases than younger age groups, which
put them at increased risk of post-burn complications and death. One-third of our patients
suffered inhalation injury in closed-space accidents.
The post-burn evolution of our cases presented no special features. The 33% mortality rate
was lower than that of elderly patients reported by other Burn Centres.
The improved survival after early excision and skin-grafting was important; in a few cases
amputation was the elective treatment. In our Burn Unit the surgical strategy in elderly
patients is two or three quick minor operations lasting only 20-45 minutes, and early
initiation of gymnastics, independently of the burn localization. As many other authorS2,
1,1 have stated, surgical therapy must be carefully planned days in advance and the
correct type of anaesthesia discussed. Local anaesthesia has been used successfully, in
correlation with light doses of morphine.
Conclusion
Elderly burn patients present
particular problems that require prevention or care by a well-organized team of physicians
of all specialities, social workers, and kinesitherapists. The impaired senses and slow
reaction times of geriatric patients tend to provoke burns of greater thickness and
extent. The skin of these patients is atrophic and the dermis thinner than in younger
patients, and their burns thus tend to be deeper. A slow rate of epidermal proliferation
leads to a decrease in healing capacity. The physiological reserves of the body and the
host immune defence mechanism are all diminished. Skin donor sites are more liable to
infection. Infected open wounds prolong decubitus and aggravate respiratory function,
which is usually already inadequate. Intensive and efficient rehabilitation is imperative
in order to prevent respiratory and vascular complications. The effective handling of
elderly burn victims is the task of a multidisciplinary team.
RESUME. Pendant les quatre
ans 1990-94, les auteurs ont traité 185 patients âgés plus de 65 ans hospitalisés dans
leur Unité de Brûlures atteints de brûlures à toute épaisseur ou de premier et second
degré en moyenne dans 26,8% de la surface totale corporelle. Dans la plupart des cas
l'étiologie était la lésion thermale (feu 63%, ébouillantement 19%, contact 10%,
friction 5%, brûlures chimiques 3%). Plus d'un tiers des accidents se sont produits à la
maison dans un environnement clos. Les lésions dues à l'inhalation étaient présentes
en 23% des patients (mortalité 100%). La mortalité complessive était 33% (âge moyen
79,7 ans contre 72,0 ans dans les patients survécus, surface corporelle brûlée moyenne
40% contre 23% dans les patients survécus). Les causes principales de la mort était les
graves complications cardiopulmonaires (70%), l'infection (18%) et le choc hypovolémique
(3%). Nos résultats nous ont persuadés que le traitement immédiat et intensif en
association avec la mobilisation précoce peut conduire rapidement à la guérison et la
rééducation de la plupart de ces patients.
BIBLIOGRAPHY
- Emke-Poulopoulou L: Demographic aging and the income
of the elderly in Greece. Social Work, 24: 221-44, 1991.
- Anous M.M., Heimbach D.M.: Causes of death and
predictors in burned patients more than 60 years of age. J. Trauma, 26: 135-9, 1986.
- Hunt J.L., Purdue G.F.: The elderly burn patient.
Am. J. Surg., 164:472-6, 1992.
- Le H.Q., Zamboni W., Eriksson E. et al.: Burns in
patients under and over 70 years of age. Ann. Plast. Surg., 17: 39-44, 1986.
- Tejerina C., Reig A., Codina J. et al.: Burns in
patients over 60 years old: epidemiology and mortality. Bums, 18: 149-52, 1992.
- Slater A.L., Slater H., Goldfarb 1W.: Effect of
aggressive surgical treatment in older patients with burns. J. Burn Care Rehabil., 10: 527-30,
1989.
| This paper was presented at the Ninth
ISBI Congress, 27 June - 1 July 1994, Paris, France and was received by MBC
on 14 March 1995. Address
correspondence to: E. Iliopoulou M.D., 3is Sept. 119, Athens 1125 1, Greece |
|