| Annals ofBurns and Fire Disasters - vol. VIII - n. 4 - December
1995
CONSIDERATIONS ON INTENSIVE CARE IN
ELDERLY BURN PATIENTS
Masellis M., D'Arpa N., Napoli B.
Divisione di Chirurgia Plastica e
Terapia delle Ustioni, Ospeclale Civico, Palermo, Italy
SUMMARY. Advanced age
is a determinant factor that inay cause death in burn patients, due to progressive
involution of the physiological functions of various organs and systems, the onset of
chronological pathological conditions, and the organism's reduced capacity to react to
therapy. These three main factors are analysed in detail, in relation to the skin and the
respiratory, cardiocirculatory, urinary and digestive systems; protein metabolism; and the
special problems of the elderly patient when subjected to burns therapy. It is of
great importance to establish the patient's general pre-burn condition. The anamnesis
should assess the degree of functionality of the main organs and systems in relation to
the patient's quality of life, the amount of physical activity usually taken, the type of
diet, and the sleeping-waking pattern. The possible chronic pathologies that should be
investigated are indicated. The three major aspects of intensive care in the elderly burn
patient are considered: the choice of infusion fluids, the rate of administration, and the
monitoring of the response.
Introduction
The number of persons aged 65 years
and over has considerably increased in the last few years and is at present increasing
still faster. It has been calculated that the phenomenon is most marked in the
over-70-year-old age group.
Increasing age leads to an increase in the likelihood of being involved in burns
accidents. This risk increases due to behavioural disturbances such as those secondary to
Alzheimer's disease and other forms of dementia, and to other conditions typical of
advanced age.
In the burn patient, age is a highly determinant additional factor that may cause death.
This is due to:
- a progressive involution of the physiological functions of
the various organs and systems
- the onset of chronological pathological conditions
- the organism's reduced capacity to react to the the~ rapies
initiated
A precise assessment of these three
aspects is fundanental for the choice of the correct form of intensive care :o be used in
the case of the burned elderly patient.
In order to give a more uniform approach to this probem, "elderly" is defined as
over the age of 65 years, i.e. .efirement age,
Involution of the physiological
functions of various organs and systems and the reduction of Physiological reserves
In elderly persons the skin tends
progressively to become trophic, dry, wrinkled, loose, and less elastic. The dermic layer
becomes thinner, there is a loss of elastic fibres and in general there is a reduction of
subcutaneous adipose tissue.
As a result, the skin's function as a protective barrier is impaired. This leads to
greater absorption of heat, so that a moderate heat source, e.g. warm water, electric
cushions or blankets, and radiators, can cause even serious physical damage. As a result
also of the reduced microcirculatory network, thermoregulation is compromised, with
increased probability of hypothermia and heat stroke. These alterations in the skin
covering assume considerable importance in the assessment of burn severity, especially in
the immediate post-burn phase. Thermal damage may appear less serious than it really
Respiratory System
Aging determines a series of modifications in the following:
Thorax, with involvement of
- the costovertebral and muscular structure with
- reduction of thoracic elasticity and
- reduction of ventilatory compliance (reduction of vital
capacity; increase of residual volume: increase of functional dead space)
Bronchi and lungs, which present
- reduction of bronchial calibre
- progressive atrophy of the bronchial mucosa with
- reduction of ciliary activity
- distension of the apical alveoli
- reduction of alveolar surfactant
- different distribution of blood flow with consequent
reduction in the cough reflex
- tendency to hypoxia
- accumulation of secretions
- increase of stasis infections
Immobilization in bed, even for just
24-72, hours tends to accentuate the reduced functioning of the respiratory system, with
the onset of fully developed conditions of bronchopulmonary pathologies due to stasis or
infection.
Cardiovascular System
The process of aging involves:
- reduction of cardiovascular function
- reduction of maximal aerobic capacity (V02 max maximum
consumption oxygen)
- reduction of cardiac muscle blood flow due to the reduced
muscular mass and to the reduction of blood flow caused by a reduction in ventricular
compliance due to the rigidity of the cardiac muscle (caused by an increase in the
connective portion and to structural modifications of the contractile proteins)
- reduction of the cardiac and vascular response to
beta-adrenergic stimulation with
- reduction of basal heart rate
- reduction of the functional reserve capacity of the
cardiovascular system in moments of stress, effort, and postural changes
- modifications of pressure values with a tendency towards
hypertension due to
- modifications of vascular capacitance secondary to
thickening of the intima and the media, increase of collagen and calcium of the clastica
and the glucosaminoglycans, increase of intimal cellularity and of lipids in the external
tunica, leading eventually to a sodium-dependent hypertrophy of the museular cells of the
media. This is associated with a modification of the sino-aortic baroceptive response to
the increase in pressure values, which triggers increased activity of the nervous
sympathetic system, with the release into the circulation of a greater quantity of
noradrenaline. This, together with the beta-adrenergic down-regulation which occurs at
cardiovascular level, contributes to the greater increase of the peripheral vascular
resistances because they facilitate the incorporation of amino acids in the proteins of
the vascular structures and thus cause thickening of the walls
If the elderly burn patient has riot led
an active physical life and is subject to long-term immobilization, the above picture is
aggravated because the following aspects are augmented:
- reduction of the organism's energy consumption
- reduction of metabolic requirements in the first days (this
may however be an advantage)
Subsequently the following may be
observed:
- increase in heart rate (caused by a diversion of the blood
flow towards the splanchnic district and also due to a reduction in the vis a tergo
determined by the cardiac muscle) failure of cardiac function to adapt to the
requirements, though reduced, with a possibility of ischaemic conditions visible on ECG
presence of ischaemic-type disturbances caused also by the reduction of K and Mg as a
result of immobilization
- onset of venous thromboses (often with pulmonary
thromboembolism) due to slowing down of blood flow, compression of the venous wall against
the base, diversion of blood towards the splanchnic system, and a tendency towards
alteration of the coagulation/fibrinolysis balance
Urinary System
After the third/fourth decade of life the following processes gradually begin:
- reduction of renal mass
- modification of intrarenal vascularization
- quantitative reduction of glomerules and tubules with
- reduction of renal plasma flow and glomerular filtration.
The glomerular filtrate and tubular mass reduce by about 6% every 10 years and at the age
of 65 years glomerular filtration is reduced by one-third
- reduction in clearance of endogenous creatinine (1
ml/min/yr) reduction in urinary excretion of creatinine (due to reduction of the muscular
mass), for which reason a constant creatinaemia value is observed despite the progressive
reduction in clearance`
In the event of prolonged immobilization
we observe:
- marked reduction in creatinine clearance secondary to
reduced muscular production and reduced endogenous creatinine
- urinary retention because the calices adopt a vertical
course with an upward flow direction, due to horizontalization of the ureters and the
difficulty of emptying the bladder (patients find it difficult to urinate in bed)
- urinary infections and urolithiasis due to an increase in
calcinuria and modifications in urine Ph caused by immobilization"
Digestive System
The process of aging affects the digestive systems in a number of ways:
- This thesis is supported by studies on acute post-burn
organ failure which have shown a clear relationship between advanced age and the
probability of the development of acute organ failure and therefore death. The situation
deteriorates further in the case of elderly persons who take little physical exercise or
worse still if compelled to stay in bed, even if only for a few days. Geriatric
specialists confirm that in these conditions important metabolic alterations occur which
must be con
- reduction of secretory and motor function (lazy sidered
carefully in the elderly bum patient. intestine)
- anorexia due to reduction of energy consumption, which
leads to early reduction of appetite and even a sense of repugnance towards food; some
drugs, e.g. digitalis, may also be responsible for anorexia
- stipsis due to reduced food intake and food quality
(semiliquid foods without roughage are often preferred), reduced physical activity,
hypotonia of the prelum abdominale caused by electrolytic alterations, especially in
potassium
- confusional state, due also to the condition of hyper
ammonaemia caused by the stasis of facces in the colon
- scatomas due to dehydration of the facces
- faecal incontinence due to scatomas which irritate the
colon mucosa, producing mucus. At the same time the putrefactive microbic fauna attacks
and liquefies recent faecal mass, producing semiliquid material which slips along the
walls and exits in the form of alvine mucose discharges alteration of hepatic function due
to
- reduced liver mass
- reduced blood flow
- reduced efficiency of the microsomial oxidation system
- reduced enzymatic activity
Physiological Functions - Physiological
Reserves
The deficiencies of these functions do not always reach a clinical threshold but may
become evident as soon as there are conditions of stress.
In such conditions the appearance of deficiencies is favoured by a reduction in the
neuroendocrine response, which is related to a drop in the concentration of hormones and
hormone receptors in the general context of physiological and endocrinal decay due to
aging. The decrease of visceral functions is more marked as age advances. When an elderly
person suffers a burn the Jecrease becomes a factor provoking death, and is there fore an
indirect index of metabolic efficiency.
- Glucose metabolism
The process of aging produces a reduced
tolerance of glucose, starting in the third decade of life. The effects of age on glucose
metabolism are evident in the altered response to tests with orally administered glucose
which have shown a mean increase in glycaemia of about 6-13 mg/dI for every decade of life
one to two hours after administration.
The causes of this phenomenon include the
following: a glucose-induced delay in secretion of insulin; a delay in the insulin-induced
inhibition of hepatic glucose output; an alteration of the peripheral utilization of
glucose in insulindependent tissues (mainly musculoskeletal); and an alteration of the
utilization of glucose in non insulin-dependent tissues (mainly CNS)."
After 24-72 hours of complete
immobilization in bed, even in young persons, there is a significant reduction in the
peripheral uptake of glucose caused by insulin resistance, as testified by the increase in
insuliDaemia levels and by the lower reduction in glycaemic levels after administration of
exogenous insulin.
One of the causes of this condition is the
lack of physical activity, which undoubtedly has an insulin-like function or at least a
functional synergism with the action of insulin.
- Protein metabolism
Elderly persons present a state of:
- hypoproteinaemia, favoured by poor feeding, digestive
disturbances and any renal malfunction
- hypopotassiaemia, favoured by an inappropriate diet,
insufficient muscular activity, and insufficient renal function
- hypomagnesia, due to nutritive deficiencies
- hypernatraemia and hyperosmolarity, due to dehydration,
hypopotassiaernia, and insufficient renal function
Reduced muscular activity and immobility
cause an increase in the urinary elimination of nitrogen, potassium, phosphorus and
calcium, causing further deterioration of the above deficits.
- Fat metabolism
Reduced physical activity in the elderly
determines a significant increase in total lipaemia, cholesterolaemia and the beta-alpha
lipoprotein ratio.
B. Onset of chronological pathological
conditions
Given the above considerations, in the
intensive care of the elderly burn patient the following are of particular importance:
- a hypothetical assessment of the patient's pre-burn
conditions as a function both of age and of possible acute pathological episodes
- an assessment of the seriousness of chronic pathological
conditions present on admission to hospital
Only an accurate anannesis, involving
family members if necessary, can make it possible to establish the patient's general
pre-burn conditions.
The anamnesis will attempt to assess the
degree of functionality of the main organs and systems in relation to the quality of life
led by the patient, the amount of physical activity taken, the type of diet, the
sleeping-waking pattern, etc.
An investigation will also be made with
regard to any pathological episodes in the following:
- respiratory system: bronchopulmonary episodes and their
frequency, pulmonary embolisms, etc.
- cardiovascular system: episodes of coronary failure,
hypertension, and cerebrovascular incidents
- urogenital system: infections of the urinary tract and
their frequency
- previous surgical operations
- long-term pharmacological treatment
The possible chronic pathologies to be
identified on admission include:
- diseases of the metabolism: diabetes, uricaernia,
hypercholesterolaernia
- tabacosis, alcoholism, addiction to narcotics
- chronicized allergies to drugs and foods
- respiratory pathologies: chronic bronchitis, asthmatic
bronchitis, bronchiectasis, etc.
- cardiocirculatory pathologies: hypertension stabilized
around values of 160/100, dilatative ischaernic cardiopathies with anginoid episodes,
terations in rate and conduction, cerebral and arteriosclerotic vasculopathies, venous
pathologies, etc.
- pathologies of the genitourinary system: chronic renal
failure, dialysis, urinary infections due to prostate hypertrophy, urolithiasis haernatic
pathologies: haemocoagulation alterations whether primary or secondary to pharmacological
treatment, anaemia, etc.
- pathologies of the digestive system: chronic diarrhoea,
stipsis, spastic colitis, hepatic failure, bile stones, cirrhosis, etc.
- neuropsychiatric pathologies: epilepsy, Parkinson's
disease, depressive neurosis, psychosis, etc.
- pathologies of the skin, muscles or skeleton: ulcers,
pressure sores, necrosis, arthropathies, etc.
- isolated or metastatic neoplastic pathologies
- multiple pathologies involving one or more organs
C. The elderly patient's capacity to
react to therapy
In burns there is no doubt that the
manner of administering therapy, especially in the acute phase, will condition prognosis.
As already said, the elderly patient has reduced cardiovascular responses and reserves
that are compromised by age, for which reason fluid therapy in intensive care can itself
be risky.
Thus a burn of fairly limited extent and
with a normal~ ly favourable prognosis can become lethal if it determines an overload of
liquids, not simply on its own account but because of the specific cardiocirculatory
system and in the antidiuretic phase of shock.
It therefore follows that in the elderly
burn patient the rate of fluid administration must have different characteristics from
those normally observed.
At this point we may consider another
important aspect in the treatment of the elderly burn patient: that of clinical
pharmacology.'
In the elderly there are a number of
pharmacokinetic modifications at the following levels:
- phase of absorption. This is modified only in part but
significantly
- phase of distribution. Owing to the reduction of the lean
mass, hydric pool, systemic flow and portal flow, this determines:
- increased distribution of liposoluble drugs
- reduced distribution of hydrosoluble drugs
- increase in the free concentration of acid drugs
- reduction in the concentration of basic drugs
- phase of elimination reduction in drug elimination rate due
to the reduced cardiac output and reduced renal vascularization, with consequent reduced
plasma flow and glomerular filtration
This involves a risk of: toxicity, in the
case of drugs with a limited therapeutic range, e.g. digoxin, chinidine, aminoglycols,
etc.
accumulation, in the case of drugs such as
penicillin, procainamide, etc.
Intensive care in elderly burn patients
On the basis of the above remarks
three aspects appear to be of major importance:
- choice of infusion fluids
- rate of administration
- monitoring of response
Infusion fluids
Intensive care in the acute burn phase is
principally concerned with the control of oedema. The increase of oedema is affected by
the quality and quantity of fluids infused.
On the basis of the assumption that the
elderly patient presents a basic hypoproteinaemia, an often precarious hydroclectrolytic
balance, and imperfectly efficient cardiocirculatory, respiratory and renal functions, the
use of colloid solutions is the most indicated choice in intensive-care.
The advantages which colloid solutions
determine as regards cardiac output, vascular and pulmonary resistance and the control of
organ and general oedema make it possible, with a smaller quantity of fluid, to restore
the circulating volume, tissue perfusion and good haemodynan-ric stability.
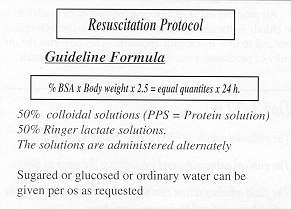
Rate of admimistration
Experience gained in the treatment
of 126 elderly patients with bums in 15 to 60% BSA enables us to make the following
considerations:
- elderly patients require a differentiated care protocol
- the use of fixed formulae to calculate the quantity of
fluid to infuse is scarcely compatible with the realistic approach of guided therapy
- the rate of administration is not regulated in terms of
fixed time (e.g. half quantity in first 8 hours, etc.) but must depend on a constant
assessment of the clinical picture and laboratory findings" (Fig. 1)
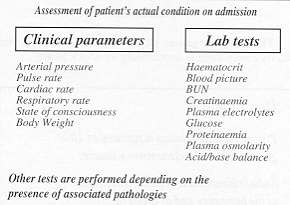
Monitoring of response
Monitoring of the functions of the
various organs and systems must be as comprehensive as possible, starting from the moment
of admission, before initiating fluid therapy, in order to assess the "actual
state" of the patient and thus to obtain "the basis on which to operate" (Fig.
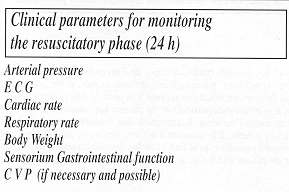
2). Monitoring must continue regularly throughout the course of treatment (Fig. 3).
On admission the clinical data and laboratory tests indicated in the slide must be
performed. The pattern of administration used in the first 24 hours is shown.
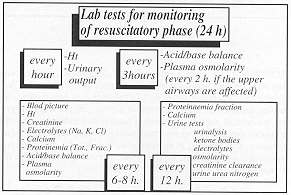
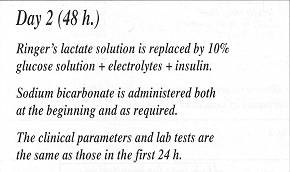
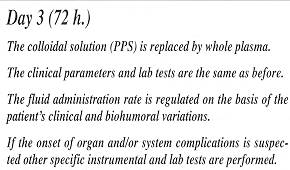
Monitoring during fluid therapy in intensive care is articulated in various time
intervals: 48 hours and 72 hours (Fig. 4).
 |
 |
| Fig.
4 |
|
Conclusions
The most dangerous phase in the
treatment of the elderly burn patient is undoubtedly the shock phase.
Intensive care is a delicate moment during which it is difficult to achieve a correct
balance between the patient's resuscitatory requirements determined by the state of
hypovolaemic shock and the capacity of the aged organism to respond.
Fluid therapy must be limited, using only sufficient quantities of fluid strictly
necessary to maintain a good clinical response.The quantity to be administered depends on
the clinical response and on laboratory findings.Generally speaking, as the fluid
requirements in most patients are only moderate, they should receive a sufficient amount
of fluid, if possible in part orally and in part venously, to maintain adequate tissue
perfusion.While the best way of measuring the adequacy of intensive care may still be
controversial, it should be remembered that changes in central venous pressure, for
example, prove more useful if followed up rather than being taken as a sign of the
beginning of pulmonary oedema. The changes are unreliable as an indicator of fluid
overload in the acute phase.All progress made in reducing the post-bum death rate in the
elderly is the result of a reduction in iatrogenic complications and to new therapeutic
measures. This confirms the difficulty of producing a standardized intensive care
protocol.
RESUME. L'âge
avancé est un facteur déterminant qui peut causer la mort des patients brûlés, à
cause de l'involution progressive des fonctions physiologiques des divers organes et
systèmes, de l'instauration de conditions pathologiques chronologiques, et de la
capacité réduite de l'organisme de réagir à la thérapie. Les auteurs analysent ces
trois facteurs en détail par rapport à la peau et aux systèmes respiratoire,
cardiocirculatoire, urinaire et digestif; au métabolisme protéique; et aux problèmes
particuliers du patient âgé soumis à la thérapie des brûlures. Il est très important
d'établir les conditions générales du patient avant l'accident. L'anamnèse doit
évaluer le degré de fonctionnalité des organes et systèmes principaux par rapport à
la qualité de vie du patient, à la quantité d'activité physique quotidienne, aux
habitudes alimentaires, et au rythme veille/sommeil. Les pathologies chroniques possibles
qu'il faut chercher sont indiquées. Les auteurs concluent en considérant les trois
aspects plus importants de la réanimation du patient âgé brûlé: le choix des fluides
d'infusion, le rythme d'administration, et le monitorage de la réponse.
BIBLIOGRAPHY
- Cadier M.A., Shakespeare P.G.: Burns in octogenarians.
Burns, 21:200-4, 1995.
- Harper R.D., Dickson W.A.: Reducing the bum risk to elderly
persons in residential care. Bums, 21: 205-8, 1995,
- Bing-Guo Li, Wei-Sha Hsu, Tsi-Siang Shih: Causes of death
in aged bum patients: analysis of 36 cases. Burns, 16: 2071-10, 1990.
- Boldoni E.: "L'assistenza geriatrica: concetti e
tecniche di prevenzione e recupero." Piccin, Padova, 1986.
- D'Arpa N., Napoli B., Masellis M.: The influence of a
variety of parameters on the outcome of the bum disease in elderly patients. Ann. Medit.
Burns Club, 6: 15-19, 1993.
- Baux S., Minoun M., Saade H., Lioret N., Esteve M., Nolland
X.B.,Berti6re N.: Burns in the elderly. Burns, 15: 239-40, 1989.
- Marchetta F., Costa F.V., Ambrosioni E.: La terapia
farmacologica dell'anziano. Medicine Illustrated, 3: 337-52, 1987.
- D'Arpa N., Napoli B., Masellis M.: Epidemiology and
prevention of burns at geriatric age. Ann. Medit. Bums Club, 5: 11-14, 1992.
- Tejerina C., Reig A., Codina J., Saforit J., Mirabet J.:
Burns in patients over 60 years old. Bums, 18: 149-52, 1992.
- Gilchrest B.A.: Age-associated changes in the skin. J. Am.
Geriatr. Soc., 30: 139-43, 1982.
- Staley M.J., Richard R.L.: The elderly patient , with
burns: treatment consideration. J. Burn Care Rehabil., 14: 559-65, 1993.
- Zoch G.: Meissl G., Bayer S., Kyral E.: Reduction of the
mortality rate in aged burn patients. Bums, 18: 153-6, 1992.
- Frad~ G.: La protratta immobilita a letto nell'anziano.
Ricerca e salute, 2: 16-19, 1990 / 3: 20-25, 1990.
- Agarwal N., Petro J., Salisbury R.E.: Physiologic profile
in burned patients. J. Trauma, 23: 577-83, 1983.
- Wright I.S.: Venous thrombosis and pulmonary embolism in
the elderly. In: Reichel W., Ed., "Clinical aspects of aging", 96-101, Williams
and Wilkins, 2nd ed., 1983.
- Cuthberton D.P.: The influence of prolonged muscular rest
on the metabolism. Biochem J., 23: 1932-8, 1929.
- Jackson R.A.: Mechanism of age-related glucose
intolerance.Diabetes care, 13th Suppl., 2: 9-19, 1990.
- Coppola L., Verrazzo G., D'Onofrio F.: Sindrome da
immobilizzazione in etA senile. Aspetti metabolici. Feder. Medica, 2: 41-5, 1995.
- Cavalieri U. Quadri A., Tammaro A., Baldoli C.: La
patologia, da immobilizzazione nel soggetto anziano. Giorn. Geront_ Suppl. 28, 1962.
- Solomon L.R., Lye M.: Hypernatraernia in the elderly
patient.Gerontology, 36: 171-9, 1990.
- Coppola L., Giuma R., Grassia A., Verrazzo G., Tirelli A.,
Torella R.: OsmolalitA plasmatica in soggetti ultraottantenni. Giom. Geront., 39: 669-74,
1991.
- Burke J.F.: Fluid therapy to reduce morbidity. J. Trauma,
19: 865-6, 1979.
Pruitt B.A. Jr: The effectiveness of
fluid resuscitation. J. Trauma, 19: 868-70, 1979.
This paper was
received on 4 April 1995, and presented at the Round Table on "Consideration on
Reanimation Therapy in Elderly Burn Patients" at the 6th EBA Congress in Verona, 13 -
15 Sept. 1995.
Address correspondence to: Prof. Michele Masellis
M.D., Divisione di Chirurgia Plastica e Terapia delle Ustioni, Ospedale Civico, Via C.
Lazzaro, 90127, Palermo, Italy. |
|