| Annals ofBurns and Fire Disasters - vol. VIII - n. 4 - December
1995
CD36 IS ONE OF THE IMMUNOLOGICAL MARKERS
EXPRESSED BY KERATINOCYTES IN ACTIVE HYPERTROPHIC SCARS
Castagnoli C.,(1) Stella M .,(2)
Menegatti E,(1) Trombotto C.,(1) Calcagni M.,(2) Magliacani G .,(2) Teich Alasia S.
' (2,3) Alessio M.(4)
1 Centre for Immunogenetics
and Experimental Oncology, CNR, Turin, Italy
2 Department of Plastic Surgery and Burn Unit, Trauma Centre, Turin
3 Piedmont Burn Studies and Research Foundation, Turin
4 DIBIT, San Raffaele Scientific Institute, Milan
SUMMARY. The
pathogenesis of hypertrophic scars is largely unknown, although there is considerable
evidence to suggest that many of its features are analogous to inflammatory dermatoses,
such as psoriasis, scleroderma and lichen planus. An aberrant expression of HLA Class 11
and ICAM-1 molecules on keratinocytes is reported in these forms of dermatosis. We have
already demonstrated in hypertrophic scars that these activation markers are ectopically
present in all layers of the epidermis. Here we show that CD36, a membrane glycoprotein
normally expressed on platelets, monocytes and endothelial cells, is expressed on
epidermal keratinocytes in the stratum granulosurn and stratum spinosum of active
hypertrophic scars but not in normotrophic scars or normal skin. These resulis, combined
with the local alteration of the biosynthesis of some cytokines in hypertrophic scars and
the ectopic expression of HLA 11 and ICAM- I molecules on keratinocytes and
fibroblasts in the tissue involved, are consistent with a pivotal role of an altered
cellular immune response in this disease.
Introduction
The pathogenesis of hypertrophic scars
remains controversial. These scars are characterized by hyperproduction of collagen for an
extended period of time, hyperplasia and increased cell turnover.' It has recently been
suggested that immunological factors may play a major role in the normal processes of
wound healing and tissue remodelling.' A disruption of these mechanisms is thought to be
involved in pathological wound healing, as in certain forms of dermatosis, e.g. lichen
plarms, scleroderma and psoriasis. Several immunological abnormities are reported in these
dermatoses, including the anomalous expression on keratinocytes of HLA DR, ICAM-I and CD36
molecules
We have already demonstrated that in hypertrophic scars the tissue involved contains an
increased number of activated T lymphocytes (70% of infiltrates) compared to normotrophic
scars (35% of infiltrates) .6 In a recent work it has been shown that in hypertrophic
tissues there is a local alteration in the biosynthesis of some cytokines.1,1 The
anomalous expression of HLA DR and ICAM-1 (CD54) molecules on keratinocytes and
fibroblasts in hypertrophic tissues has also been demonstrated.
CD36 is an 88 kDa membrane glycoprotein expressed by the erythrocyte precursors, mature
monocytes, platelets, endothelial cells of the microvasculature, and mammary epithelial
cells. In platelets this molecule has been shown to serve as the receptor for two
extracellular matrix proteins, collagen and thrombospondin I." Additional aspects of
CD36 are as follows: i) it is expressed by macrophages involved in phagocytosis of
neutrophils and CD4+ and CD8+ T-lymphocytes undergoing apostosis;1 1,12 ii) it is a
receptor for oxidized low-density lipoprotein on macrophages; 11 iii) it is implicated in
the binding and transport of fatty acids by foam cells.
The role of CD36 as a cell surface receptor has been extended to a signal transduction
molecule in platelets and monocytes, being associated in platelets to protein tyrosine
klinases of the pp60-,,, gene family.
In this study we investigate the expression of CD36 molecules in hypertrophic scars and
their correlation with other activation markers previously demonstrated to be ectopically
expressed on keratinocyles. We also analyse the correlation between CD 36 and other
classic markers of macrophages and dendritic cells in the tissues involved.
Materials and methods
Patients
Biopsies were taken after informed
consent from 25 patients (15 women and 10 men, aged 23-60 years) subjecled to plastic
surgery under general anaesthesia for the correction of extensive hypertrophic scars
consequent to thermal injury. The burned surface area (BSA) of the patients corresponded
to 10-40% of the body.
Hypertrophic scars were still present at least one year post-trauma despite continuous
compressive therapy, massage and physiotherapy. The scars were raised, erythematons, and
often painful, with variable degrees of skin retraction affecting articular motility; at
the surface they showed telangectasies, little bullae and sometimes trophic ulcers. The
overall judgement was that they were active lesions with no sign of regression.
Control samples included five specimens of normal skin taken from patients undergoing
corrective plastic surgery procedures, and ten specimens of normotrophic scars from
informed consent patients undergoing surgery for reconstructive purposes.
Tissue specimens
Five-millimeter punch biopsies of hypertrophic scars and controls were obtained from
different anatomical sites of the body. Tissue samples were snap-frozen in cold isopentane
(-70 'C) and mounted in OCT 4583 embedding compound. Five-micron-thick cryostat sections
were cut in serial sections and transferred to microscope slides. The slides were
air-dried and stored at -80 'C.
Monoclonal antibodies (MoAb) and
conventional antisera
The monoclonal antibodies used in this work were: the anti-CD36 MoAb NL07 (IgM);" the
anti-HLA-DR, DP MoAb Hot 214 (IgGI), the anti-HLA-DR, DP, DQ MoAb AA3.84, the anti-ICAMA
MoAb CL203.4, and the V1727516 [1 and references therein]; the anti-CD 11 c MoAb Leu M5
(lgG2b, Becton~Dickinson); the anti-CD11b MoAb OKM1 (IgGI, Ortho-Diagno sties); and the
anti-CD1a MoAb OKT6 (lgGI, Ortho-Di agno sties). Rabbit antimouse lg and
peroxidase-conjugated swine anti-rabbit lg were from Dakopatts, Copenhagen, Denmark.
Immunoenzymatic staining procedures
Sequential tissue sections were incubated with MoAb and stained using a three-stage
immunoperoxidase reaction (PAP) as previously described.' MoAb were titrated so as to
yield maximal specific staining and minimal non-specific or background staining.
Endogenous peroxidase activity was inhibited by the addition of methyl alcohol and 0.033%
hydrogen peroxide. The specificity of the immunostaining was evaluated by replacing the
primary antibody with non immune ascites. Slides were examined double-blind.
Results
Serial sections of hypertrophic scar
biopsies from 25 patients, plus sections of normotrophic scar biopsies from ten
individuals and five specimens of normal skin, were stained with anti-CD36, anti-ICAM-1,
anti-HLA Class 11, anti-CD1 lb, anti-CD1 lc and CD1a with a three-stage immunoperoxidase
reaction.
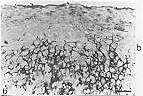
All hypertrophic scar samples showed strong positivity for the CD36 antigen in suprabasal
keratinocytes, in particular in the stratum granulosum and stratum spinosum of the
epidermis (Figs. ]a, b). The reactivity of the antiCD36 MoAb was sometimes
localized in foci in these strata (Fig. 1b). CD36 immunoperoxidase staining was
always negative in the basal layer of epidermis and in the stratum corneum (Figs. ]a,
b). The pattern of CD36 expression was not dependent on the thickness of the epidermal
layer observed in different scar samples.
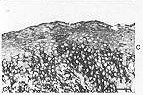
In all tested serial sections of hypertrophic scars, the reactivity pattern of anti-CD36
MoAb was not comparable to the pattern of anti-HLA Class 11 and anti-ICAM-1 MoAbs (Figs.
2a, b, c). The HLA Class 11 and ICAM-1 antigens were highly expressed on the
keratinocyte cell membrane in the basal layer and sometimes in the mid~epi~ dermal zone (Figs.
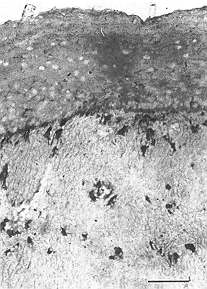
2a, b), while their expression decreased in the upper layers of epidermis.The CD 1 lb
antigen, a known macrophage marker, was never found on keratinocytes of any epidermal
layers (Fig. 3). Similar results were obtained when anti-CD I I c MoAb was used
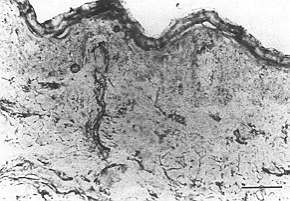
(data not shown).In the dermis of all tested hypertrophic scar samples, CD36+ cells were
more abundant than in normotrophic scars and normal skin biopsies. CD36+ cells were widely
distributed in the subpapillary compartment and in reticular dermis (fig. 4). The
immunoreactivity pattern of anti-CD36 MoAb was very similar to patterns seen in serial
sections stained with anti-CD11b and CDD I I c MoAbs (Fig. 3). In the dermis of
hypertrophic scar samples, the CD36 antigen was also expressed on endothelial cells of the
microvasculature (Fig. 4). The vascular endothelial cells, in addition to the
expression of CD36 molecules, showed strong reactivity with anti HLA Class 11 and
anti-ICAM-1 MoAbs (data not shown). Scattered epidermal-branched Langerhans-like cells
(DR+ and CD I a+) found in serial sections of hypertrophic scars did not express CD36
antigens (data not shown). Normal skin and normotrophic scar biopsies were exa mined as
control. In contrast to hypertrODhic scar samples.
CD36 molecules were not detected in the
epidermis in normotrophic scar samples (Fig 5). In normal skin sections the reactivity
pattern of anti-CD36 MoAb was identical to that seen for normotrophic scar samples. Table
I summarizes the results of MoAb reactivity on nonhaematopoietic cells.
Discussion
The results presented in this work
show that CD36 is ectopically expressed on keratinocytes of hypertrophic scars as in other
skin pathologies such as psoriasis, lichen planus and pemphigus vulgaris. These data
further support our hypothesis of an involvement of the immune system in hypertrophic
scarring.
A recent interesting work has reported that when normal keratinocytes are treated in vitro
with g-interferon (gIFN) they express the same molecules (ICAM-1, HLADR) that are observed
in hypertrophic sear tissues and they are also capable of providing co-stimulatory signals
to T cells .21 These keratinocytes, seem to play a fundamental role as accessory cells,
delivering co-stimulatory signals to T cells engaged by antigens or superantigens and
influencing the development of different T cell immune responses.
It is tempting to speculate that also in hypertrophic scarring the CD36, DR and ICAM-1
molecules" expressed on keratinocytes might act as co-stimulatory molecules
recruiting and activating T cells. In hypertrophic sear bi-
| Tissue |
Cell types |
CD36 |
ICAM- I |
HLA C1 II |
CD11b |
CD11c |
Hypertrophic scars
(N'=25) |
Keratinocytes |
Basal layer |
- |
+ foci |
+ |
- |
- |
" |
Stratum spinosum |
+ |
+ |
+ |
- |
- |
" |
Stratum granulosurn |
+ |
+/- |
+/- |
- |
- |
" |
Upper layers |
- |
- |
- |
- |
- |
Fibroblasts |
|
- |
+ |
+ |
- |
- |
Endothelia |
|
+ |
+ |
+ |
+ |
+ |
Normotrophic scars
(N'= 10) |
Keratinocytes |
All layers |
- |
- |
- |
- |
- |
Fibroblasts |
- |
- |
- |
- |
- |
Endothelia |
+ |
+ |
+ |
ND |
ND |
Normal skin
(N'=5) |
Keratinocytes |
All layers |
- |
- |
- |
- |
- |
Fibroblasts |
- |
- |
- |
- |
- |
Endothelia |
+ |
+ |
+ |
ND |
ND |
|
| Table I - Expression of CD36, ICAM-1, HLA Class II, CD 1 lb
and CD 1 le antigens by nonhaematopoietic cells in hypertrophic scars and controls opsies
the presence of a considerable amount of infiltrating dermal macrophages expressing CD36
molecules and the expression of activation markers on endothelial cells indicate moreover
that there is an ongoing active inflammatory response. Cytokines such as 9-IFN or TNF(x
released from activated infiltrating cells, which are widely present in involved tissue 6
could therefore promote the expression of CD36 and other accessory antigens in
hypertrophic scar keratinocytes. |
|
It has to be
underlined that the expression of HLA DR, ICAM-1 and CD36 molecules is not comparable:
CD36 is detected only in the stratum granulosum and stratum spinosum while the others are
detected in all epidermal layers. The different expression pattern of CD36, HLA class II
and ICAM-1 could suggest that keratinocytes in hypertrophic scars evolve through
sequential stages of differentiation, probably playing different roles in the immune
response in scars.
In conclusion, in hypertrophic scars the ectopic expression on keratinocytes of HLA class
11, ICAM-1 and CD36 molecules suggests a cross-talk with the immunocompetent cells,
underlying the involvement of the immune system in pathological scarring. However, the
regulation of the ectopic expression and the role of CD36 antigen in keratinocytes of
hypertrophic scars still remain to be defined.
RESUME. La
pathogenèse des cicatrices hypertrophiques n'est pas bien connue, même si les évidences
indiquent que beaucoup de ses aspects charactéristiques sont analogues à celle des
dermatoses inflammatoires, comme le psoriasis, la sclérodermie et le lichen planus. Dans
ces formes de dermatose une expression aberrante des molécules HLA de classe Il et ICAM-1
sur les kératinocytes a été observée. Dans les cicatrices hypertrophiques nous avons
déjà démontré que ces marqueurs de l'activation sont présents ectopiquement dans
toutes les strates de l'épiderme. Ici nous montrons que la CD 36, une glycoprotéine
membraneuse normalement exprimée sur les plaquettes, les monocytes et les cellules
endothéliales, est exprimée sur les kératinocytes épidermiques dans le stratum
granulosum et le stratum spinosum des cicatrices hypertrophiques actives mais non dans les
cicatrices normotrophiques ou la peau normale. Ces résultats, alliés à l'altération
locale de la biosynthèse de certains cytokines dans les cicatrices hypertrophiques et
l'expression ectopique des molécules HLA Il et 1CAM-1 sur les kératinocytes et les
fibroblastes du tissu intéressé, sont compatibles avec un rôle central d'une
immunoréponse cellulaire altérée dans cette maladie.
Acknowledgements. This
work was supported by the Fondazione Piemontese per gli Studi e le Ricerche sulle Ustioni
(Piedmont Burn Studies and Research Foundation). Dr C. Castagnoli was supported by a
fellowship from the same Foundation. We thank Dr G. Ponzio for his help with the
photomicrographs and Dr R. Sitia for his critical reading of the manuscript.
BIBLIOGRAPHY
- Stella M., Castagnoli C., Magliacani G.,
Richiardi P.: Fisiopatologia delta cicatrizzazione patologica (revisione bibliografica).
Riv. Ital. Chir. Plast., 21: 199-208, 1989.
- Janssen de Limpens A.M.P., Cormane R.H.: Studies
on the immunologic aspects of keloid and hypertrophic scars. Arch. Dermat. Res., 274:
259-64, 1982.
- Vejlsgaard G.L., Ralfkiaer E., Avnstorp C.,
Czajkowski M., Marlin S.D., Rothlein R.: Kinetics and characterization of ICAM-1
expression on keratinocytes in various inflammatory skin lesions and malignant cutaneous
lymphomas. J. Am. Acad. Dermatol., 20: 782-92, 1989.
- Griffiths C.E.M., Voorhees J.J., Nickoloff B.J.:
Characterization of ICAM-1 and HLA-DR expression in normal and inflamed skin:modulation by
recombinant gamma interferon and tumor necrosis factor. J. Am. Acad. Dermatol., 20:
617-24, 1989.
- Lisby S., Ralfkiaer E., Hansen E.R., Vejlsgaard
G.L.: Keratinocyte and epidermal leukocyte expression of CD36 (OKM5) in benign and
malignant skin diseases. Acta Derm. Venereol., 70: 18-22, 1990.
- Castagnoli C., Stella M., Berthod C., Magliacani
G., Momigliano Richiardi P.: TNF production in hypertrophic scarring. Cell Immunol., 147:
51-4, 1993.
- Castagnoli C., Stella M., Magliacani G., Richiardi P.: The
role of TNF alpha and beta cytokines in scar hypertrophy in bum patients: an
immumohistochemical study. Ann. Medit. Burns Club, 8: 23-7,1995.
- Peruccio D., Castagnoli C., Stella M., D'Alfonso S.,
Momigliano Richiardi P., Magliacani G., Teich Alasia S.: Altered biosynthesis of TNF alpha
is involved in post-burn hypertrophic scars. Burns, 20: 118-21, 1994.
- Castagnoli C., Stella M., Magliacani G., Teich Alasia S.,
Momigliano Richiardi P.: Anomalous expression of HLA class 11 molecules on keratinocytes
and fibroblasts in hypertrophic scars consequent to thermal injury. Clin. Exp. Immunol.,
82: 350-5, 1990.
- Castagnoli C., Stella M., Magliacani G., Ferrone S.,
Momigliano Richiardi P.: Similar ectopic expression of ICAM- I and HLA Class 11 molecules
in hypertrophic scars following thermal injury. Bums, 20: 430-3, 1994.
- Greenwalt D.E., Lipsky R.H., Ockenhouse C.F., Ikeda H.,
Tandon N.N., Jamieson G.A. ~ Membrane glycoprotein CD36: a review of its roles in
adherence, signal transduction and transfusion medicine. Blood, 80: 1105-15, 1992.
- Savill J., Hogg N., Ren Y., Haslett C.: Thrombospondin
cooperates with CD36 and vitronectin receptor in macrophage recognition of neutrophils
undergoing apoptosis. J. Clin. Invest., 90: 1513-22, 1992.
- Akbar A.N., Savill J., Gombert W., Bofill M., Borthwick
N.J., Whitelaw F., Grundy J.E., Janossy G., Salmon M.: The specific recognition by
macrophages of CD8+, CD45RO+ T cells undergoing apoptosis: a mechanism for T-cell
clearance during resolution of viral infections. J. Exp. Med., 180: 1943-7, 1994.
- Endemann G., Stanton L.W., Madden K.S., Bryant C.M., White
R.T., Protter A.A.: CD36 is a receptor for oxidized low density lipoprotein. J. Biol.
Chem., 268: 11811-6, 1993.
- Abumrad N.A., EI-Maghrabi M., Amri E., Lopez E., Grimaldi
P.A.:Cloning of a rat adipocyte membrane protein implicated in binding or transport of
long-chain fatty acids that is induced during pre-adi pocyte differentiation. J. Biol.
Chem., 268: 17665-8, 1993.
- Alessio M., Greco N.J., Primo L., Ghigo D., Bosia A.,
Tandon N.N., Ockenhouse C.F., Jamieson G.A., Malavasi F.: Platelet activation and
inhibition of malarial cytoadherence by the anti-CD36 IgM monoclonal antibody NL07. Blood,
82: 3637-47, 1993.
- Ockenhouse C.F., Magowan C., Chulay J.D.: Activation of
monocytes and platelets by monoclonal antibodies or malaria-infected erythrocytes binding
to the CD36 surface receptor in vitro. J. Clin. 24.Invest., 84: 468-75, 1989.
- Trezzini C., Jungi T.W., Spycher M.O., Maly F.E., Rao P.:
Human monocyte CD36 and CD16 are signaling molecules. Evidence from studies using antibody
-induced chemiluminescence as a tool to probe signal transduction. Immunology, 71: 29-37,
1990.
- Alessio M., Ghigo D., Garbarino G., Geuna M., Malavasi F.:
Analysis of the human CD36 leucocyte differentiation antigen by means of the monoclonal
antibody NL07. Cell Immunol., 137: 487 500,1991.
- Barker J.N.W.N., Markey A.C., Allen M.H., MacDonald D.M.:
Keratinocyte expression of OKM5 antigen in inflammatory cutaneous disease. Brit. J. Derm:,
120: 613-8, 1989.
- Viac J., Chardonnet Y.: Immunocompetent cells and
epithelial cell modifications in molluscum contagiosum. J. Cutan. Pathol., 17: 202-5,
1990.
- Nickoloff B.J., Turka L.A.: Immunological functions of
non-professional antigen-presenting cells: new insight from studies of T-cell interactions
with keratinocytes. Immunol. Today, 15: 464-9, 1994.
- Nikoloff B.J., Mitra R.S., Green J., Zheng X-G., Shimizu
Y., Thompson C., Turka L.A.: Accessory cell function of keratinocytes for superantigens.
J. Immunol., 150: 2148-59, 1993.
- Castagnoli C., Trombotto C., Stella M., Calcagni M.,
Momigliano Richiardi P., Magliacani G.: Interferon garnma and interferon gamma receptor in
post-burn hypertrophic scars: is it a remission marker? Abs. VI Cong. E.B.A., 1995.
| This paper was received on 23
November 1995. Address correspondence
to: C. Castagnoli M.D.. Dipartimento di Genetica Biologica e Chimica Medica, UniversitA di
Torino, Via Santena 19, 10126 Torino, Italy. Tel.: + 11.6706664, 6933457; Fax: +
11.674040. |
NINTH MEETING OF
MBC
28 May - 1 June 1996
Tunis
Main Topics:
Burns: Prevention and sequelae
Prevention of fire disasters
Scientific secretariat:
H6pital Aziza Othmana
Place de la Kasbah 1008 Tunis, Tunisia
Tel.: (216-1) 263-904 / 663-640
Fax: (216-1) 563-971 |
|