| Annals of Burns and Fire Disasters - vol. VIII - n. 4 - December
1995
SOFT TISSUE RECONSTRUCTION OF THE BURNED
HAND
Atiyeh B.S., Saba M.
American University of Beirut Medical
Center, Beirut, Lebanon
SUMMARY. The burned
hand represents a real therapeutic challenge because of its particular anatomy and its
intricate function. An algorithm for soft tissue reconstruction of acute hand burns and
repair of late contractures is presented for each of the three anatomical areas of the
hand: the palm, the fingers, and the dorsum. Spontaneous healing of deep bums in these
areas can lead to catastrophic results. Adequate skin coverage is critical for function.
Early soft tissue coverage of hand burns is emphasized in order to prevent the formation
of disabling contractures.
Introduction
The burned hand represents a real
therapeutic challenge because of its particular anatomy and its intricate function. Bums
of the hand are a special case and are categorized as major injuries by the American Burn
Association.
For the sake of presentation, the hand can be divided anatomically into three main areas:
1. the palm
2. the fingers
3. the dorsum
Each of these areas has its own
characteristics that must be dealt with. But, whatever the case, preservation of hand
function must always be our goal and not merely simple skin coverage. It is far better to
prevent bum complications in the hand than to deal with their long-term sequelae.1
According to Robson,' "the key to making the burned hand functional is to have the
goal to prevent the need for reconstruction and rehabilitation from the outset". He
also lists six principles of the management of the acute hand bum:
1. Do no harm
2. Maintain circulation
3. Prevent infection
4. Obtain wound closure
5. Preserve or regain motion
6. Obtain functional rehabilitation
It is definitely preferable to achieve
soft tissue coverage early in order to prevent the development of contractures which with
time will be complicated by joint ankylosis and tendon shortening. Even so, we are very
often called upon to correct severe contractures resulting from secondary healing of burn
wounds.
In general, in our Mediterranean population, any burn that takes more than two to three
weeks to heal spontaneously has 80% chance of developing hypertrophic scarring and wound
contractures .4 These must be avoided at all costs in the hand. Early excision and skin
grafting are the standard therapy for the burned hand.',' Occasionally, soft tissue
coverage by split-thickness skin graft (STSG) or full-thickness skin graft (FTSG) is not
applicable, in which case flaps should be performed. The experience gained from dealing
with various hand pathologies can be satisfactorily adapted to hand burns since the
ultimate goal of preservation of form and function is the same for any hand condition.
1. The palm (Fig. 1)
The palm is the most protected area of the
hand. It is not frequently affected by burns except in children, who tend to grab hot
objects or fall on to hot surfaces such as a heating or cooking stove.
The palm is covered by thick glabrous skin with thick underlying subcutaneous fat. For
this reason, tendons are well protected in the palm and rarely get exposed, even in
full-thickness bums.
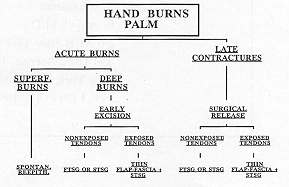
|
Fig. 1 -
Algorithm: palm of the hand bums. |
|
Burns to the palm usually tend to be
superficial and heal spontaneously by epithelial regeneration with proper topical care.
Deeper burns must be excised and the wound covered with skin graft. FTSG is superior to
STSG in this location because it has a lower potential for contracting,' although this
opinion is not shared by all workers in the field.
Skin contractures secondary to bums of the palm must be dealt with as soon as possible
with release and local Zplastics or skin grafting, particularly in a growing child in whom
these contractures may result in serious deformities.
Distant flap coverage is rarely indicated for burns of the palm except in extreme cases.
Thick flaps are definitely to be discouraged because of their poor functional and cosmetic
result. Flap coverage may become indicated following the release of long-standing severe
flexion contractures resulting in exposure of the flexor tendons in the mid palm. For such
cases a free fascia (radial forearm, temporalis or scapular) or a pedicled radial forearm
fascia covered with an STSG may be the solution. Whenever these onestage elaborate
procedures cannot be performed, a groin or an abdominal pedicled flap can be used. At the
second stage, the skin of the flap is completely detached leaving a vascular layer of fat
on the palm which will be skin-grafted.
2. The fingers (Fig. 2)
The fingers, because of their terminal
anatomical location, are at real risk in any burn of the upper extremity even if they are
not directly involved. Proper escharotomies must be performed without delay in order to
avoid ischaemia to the fingers.
When burned the extensor surface of the digits is more critical because of the superficial
location of the tendons and the bony structures. The volar surface of the fingers is well
padded and the flexor tendons are well protected, but any deep burn in this location will
cause severe flexion contracture if not attended to early.
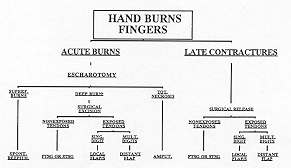
|
Fig. 2 - Algorithm:
finger bums. |
|
Skin grafts have only a minor role in
resurfacing deep finger bums except possibly on the volar surface, because in most cases
deeper structures become exposed. Such burns are best treated by flaps. An isolated finger
burn can be easily covered by a local flap, cross-finger flap or neurovascular island
flap. Burns to multiple digits will require distant flaps for soft tissue coverage.
Deep or even more superficial circumferential finger burns resulting in necrosis of the
skin envelope end up with amputation. There is little else that can be done to preserve
form and function.
The treatment of finger burn contractures and syndactyly follows the same rationale as the
treatment of acute burns. Skin grafts are used routinely together with Z-plastics or V-Y
advancement flaps.More complex flaps are needed when vital structures are exposed or in
cases of recurrent contractures.
3. The dorsum (Fig. 3)
The dorsum of the hand is covered by
soft pliable skin without any underlying subcutaneous fat. The extensor tendons are hence
at risk of exposure with any deep burn. The dorsum of the hand is often involved in bum
injuries. The palms are used to protect the face in the event of a fire, exposing the
dorsum to the flames.
Relatively superficial burns can be tangentially excised and skin-grafted. Deeper burns
require flaps for coverage. Most conventional flaps, such as groin or abdominal flaps, are
too thick and require a second-stage surgical debulking. The reverse radial forearm flap
can, whenever possible, provide excellent skin quality for the dorsum of the hand.
Microvascular composite tissue transfer has expanded our armamentarium for soft tissue
reconstruction. Possible donor sites are the contralateral radial forearm, dorsalis pedis,
scapular or temporalis areas. Free fascial flaps covered by STSG can provide excellent
cosmetic and functional results. The only drawback of the lengthy free flap procedures is
their applicability in seriously burned patients.
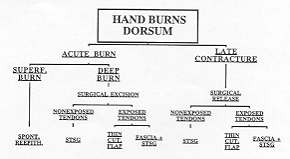
|
Fig. 3 - Algorithm:
dorsurn of the hand burns. |
|
Conclusion
If the spontaneous secondary healing
of deep burns with contraction of wound edges and re-epithelialization can be tolerated in
some areas of the body, this type of wound healing has disastrous effects on the hand. If
serious contractures are to be avoided, hand burns must be addressed as early as possible
and provided with adequate skin coverage. Satisfactory functional results of hand burns
depend on the consorted efforts of timely soft tissue resurfacing and proper splinting and
rehabilitation. The proposed algorithms can be a useful guide for all physicians,
particularly for proper referral of the hand burn. They may also be helpful for teaching
purposes.
RESUME. La main brûlée
constitue un grand problème thérapeutique à cause de son anatomie particulière et de
sa fonction compliquée. Pour la reconstruction des tissus moux dans les brûlures aiguës
de la main et pour la réparation des rétractions tardives les auteurs présentent un
algorithme pour chacum des trois zones anatomiques de la main: la paume, les doigts et le
revers. La guérison spontanée des brûlures profondes dans ces zones peut conduire à
des résultats catastrophiques. Une couverture cutanée suffisante est essentielle pour la
fonction. Les auteurs soulignent l'importance de la couverture précoce des tissus moux
pour prévenir la formation des rétractions invalidantesa.
BIBLIOGRAPHY
- American Burn Association: Guidelines for service standards
and severity classifications in the treatment of burn injury. Bull. Am. Coll. Surg., 69:
24, 1984.
- Robson M.C. et a].: Making the burned hand functional.
Clin. Plast.Surg., 16: 663, 1992.
- Parry S.W.: Reconstruction of the burned hand. Clin. Plast.
Surg., 16:577,1989.
- Deitch E.A. et al.: Hypertrophic bum scars: analysis of
variables. J. Trauma, 23: 895, 1983.
- Janzekovic Z.: A new concept in the early excision and
immediate grafting of burns. J. Trauma, 10: 1103, 1970.
- Janzekovic Z.: The dermal burn. In: Derganc M. (ed.):
"Present clinical aspects of burns: a symposium". Maribor, Mariborski Tisk, p.
215,1968.
- Rudolph R.: Inhibition of myofibroblasts by skin grafts.
Plast. Reconstr. Surg., 63: 473, 1979.
- Pensler J.M. et al.: Reconstruction of the burned palm:
full-thickness versus split-thickness grafts - long-term follow-up. Plast. Reconstr.
Surg., 81: 46, 1988.
- Tanzer R.C.: Correction of interdigital burn contractures
of the hand. Plast. Reconstr. Surg., 3: 434, 1948.
- Alexander J.W., MacMillan B.G., Martel L.: Correction of
postbum syndactyly: an analysis of children with the introduction of the VM plasty and
post-operative pressure inserts. Plast. Reconstr. Surg., 70: 345, 1982.
- Huang T.T., Larson D.L., Lewis S.R.: Burned hands.
Plast.Reconstr. Surg., 56: 21, 1975.
- Kutzman L.C., Stem P.J., Yakuboff K.P.: Reconstruction of
the burned thumb. Hand Clin., 8: 107, 1992.
- Bhattacharya S. et al.: Management of burn contractures of
the first web space of the hand. Bums, 18: 54, 1992.
| This paper was received on 21
November 1994, Address correspondence
to: B.S. Atiyeh M.D., American University of Beirut Medical Center, P.O. Box 113, 6044
Beirut, Lebanon. |
|