| Annals ofBurns and Fire Disasters - vol. VIII - n. 4 - December
1995
THE USE OF FASCIOCUTANEOUS THIGH FLAPS IN
THE RECONSTRUCTION OF GROIN AND TROCHANTERIC DEFECTS
Higazi M, Ayad H, Shalaby H.
Plastic and Reconstuctive Surgery
Unit, Tanta University, Tanta, Egypt
SUMMARY. Anterolateral and
anteromedial fasciocutaneous thigh flaps were used in the treatment of fifteen patients
suffering from postburn groin contracture. The anterolateral fasciocutaneous flap was used
to cover trochanteric bedsores in five patients. The flaps were found to be large enough
to cover extensive defects. The vascular pedicle is long with a wide are of rotation and
minimal anatomical variation. The morbidity of the donor site is acceptable.
Introduction
Post-burn contracture of the groin,
although uncommon, causes patients distressing symptoms that are difficult to treat. A
variety of different techniques are available: skin grafting, local cutaneous flaps, and
fascio- or myocutancous flaps. Roberts and Dickson' stated that skin grafting has multiple
disadvantages as it is of uncertain take and needs prolonged splinting and immobilization,
with recontracture not being uncommon. The use of local flaps is suitable only for narrow
contractures and needs sufficient normal skin around the contracted area, while it is
always insufficient. Nahai et al.' described the use of tensor fascia lata myocutaneous
flap for groin defects. Bostwick et al.' used the omentum and myoeutaneous flaps for the
repair of groin defects after ablative surgery. Wang et al.' used the medial
fasciocutaneous flap for the repair of perineum, vagina and groin defects. Hayashi and
Maruyawa,' Turley et al.' used the same flap for post-burn groin contracture. Maruyama et
al.' used the lateral thigh flap for the repair of ischial trochanteric defects.
 |
 |
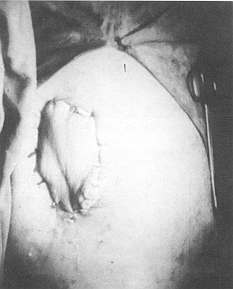
| Fig. 1 - The
design of the anterornedial fasciocutaneous thigh flap in a case of contracted groin and
axilla. |
Fig. 2 - The
vascular pedicle of the anterornedial fasciocutaneous thigh flap. |
|
In the present study we used medial and
lateral fasciocutaneous thigh flaps to cover groin and trochanteric defects.
Patients and methods
This study was performed in fifteen
patients suffering from post-bum contracted groin and five patients suffering from
trochanteric bedsores. The age range was from six to fifteen years. Fourteen patients were
female and six were male.
According to the severity of the contracture and the area of healthy skin on the thigh,
the patients with postburn contracture were treated with one of the two techniques, while
the patients with trochanteric bedsores were treated with the anterolateral
fasciocutaneous thigh flap.
Technique
Under general anaesthesia, and after
sterilization of the area with 10% povidone iodine, the recipient site was prepared by
release of the contracture in burned patients and by excision of all dead tissue in
trochanteric defects.
1. Anteromedial fasciocutaneous flap
First the design of the flap was drawn, as
shown in Fig. 1. For elevation of the flap, skin incision was started at the lower
border and continued at the medial and lateral borders. The wound was then deepened and
the deep fascia was sutured to the skin to prevent shearing movements The flap was
elevated from below, upwards and sub fascially as far as the rotation point 6-8 cm below
the inguinal ligament in the midline of the thigh, where the vascular pedicle was searched
for around the border of the sartorius muscle at the apex of the femoral triangle (Fig.
2). The flap was rotated to cover the defect either under a tunnel or directly in
severe cases. The deep fascia was fixed by Vicryl 3/0 interrupted sutures and the skin was
closed by silk sutures. The donor site was closed either pri marily or with skin grafting (Fig.
3).
The flap was designed and drawn on the thigh with the patient supine, the thigh slightly
flexed and the hip internally rotated.
2. Anterolateral fasciocutaneou s thigh flap The posterior edge of the iliotibiallract was
traced up from the lateral condyle of the femur to the greater trochanter. The vascular
supply of the skin could be detected at the middle of this line at the mid-inguinal point
(Fig. 4),
Dissection started distally and proceeded on both sides deep to the fascia. The edges
of the fascia were sutured to the skin to prevent any shearing effect. The vascular
pediele was searched for and followed proximally to lengthen the arc of rotation. It is
present at a fixed point on a line drawn from the anterior superior iliae spine to the
lateral edge of the patella. The cutaneous branch either penetrates the vastus lateralis,
in which case a cuff of the muscle has to be excised with the vessel, or it passes into
the intermuscular space.' The flap was then rotated to cover the defect and the donor site
was closed primarily or by grafting (Fig. 5).
Results
The patients were classified in four
groups on the basis of ' the severity of the contracture and the area of healthy skin
availableon the abdomen and thigh.
 |
 |
| Fig. 3 -
The flap in position and the donor site closed primarily. The contracted axilla repaired
by multiple Z-plasty. |
Fig. 4 -
The design of the anterolateral fasciocutaneous thigh flap. |
 |
 |
| Fig. 5 -
The flap transposed under skin tunnel to the recipient site. |
Fig. 6 -
Giant defect closed with anterolateral flap and split thickness skin graft. The donor site
closed primarily. |
|
* Group one: localized narrow band or web
of contracture with healthy surrounding skin
* Group two: diffuse or broad band of contracture with intact abdominal and thigh~skin
* Group three: diffuse or broad band of contracture with scarred abdominal and normal
thigh skin
* Group four: diffuse contracture with scarred abdominal and thigh skin
The post-burn patients described in this
work belonged to the first three groups. It was difficult preoperatively to predict the
Size of the defect, but after contracture release the extent ranged from 7 x 12 to 20 x 23
em. In wide defects the flap was not sufficient and split-thickness skin graft was used
either above or below the flap (Fig. 6). The vascular pedicle of the anteromedial
fasciocutaneous flap. was found at the superomedial border of the sartorius, muscle at the
apex of the femoral triangle 6-8 em from the mid-inguinal point.
The vascular pediele of the anterolateral fasciocutaneous flap was found-to be constant.
Dissection of the descending branch as far as its origin gave a long pedicle facilitating
the flap's arc of rotation. The donor site of both flaps was closed primarily in twelve
cases. In the other cases split-thickness skin graft was used to cover the donor site (Fig.
7).
The commonest complication was seroma, which was overcome by use of a Portovae suction
drainage system at the recipient site under the flap. Necrosis of the distal end of the
flap occurred in one case of anteromedial fasciocutaneous flap. This healed after
conservative treatment without surgical intervention (Fig. 8). The end results of
both kinds of flap were functionally and aesthetically good, with minimal complications
and morbidity in donor sites (Figs. 9, 10, 11).
Discussion
Turley et al.1 reports on a variety of
techniques used by different authors for the reconstruction of groin defects, none of
which is ideal, including multiple Z-plasty, local cutaneous flaps and myocutaneous flaps.
Skin grafting has several disadvantages, e.g. uncertain graft take with recontracture
requiring prolonged immobilization. Larson et al.1 and Roberts and Dickson' have found
that skin grafting commonly leads to hyperpigmentation and poor cosmetic results.
To prevent these complications, Mathes and Nahai" and Budo et al.11 preferred to use
flaps for the coverage of flexor areas. The use of muscle and myocutaneous flaps, although
suitable for covering deep defects of the groin and bedsores, as used by Bostwick et al.,I
Hill et al." and Gopinath et al.," leads to marked defects at the donor site and
a bulk at the recipient site. Ponten" and Maruyama et al.' preferred the use of
fasciocutaneous flaps to cover the defects and to prevent the drawbacks of myocutaneous
flaps.
In this work the use of the fasciocutaneous flap showed the following advantages:
- the flap is large enough, having a long vascular pedicle
with a wide arc of rotation and minimal anatomical variations.
- the dissection and raising of the flap is easy and leaves
minimal morbidity at the donor site, which is commonly a linear scar.
Fasciocutaneous thigh flaps are therefore
recommended in the treatment of groin and trochanteric defects.
RESUME. Les auteurs ont
utilisé le lambeau antérolatéral et antéromédial fasciocutané de la cuisse dans le
traitement de quinze patients atteints de contractures inguinales dues aux brûlures, et
le lambeau fasciocutané antérolatéral pour couvrir les escarres de décubitus chez cinq
patients. Les lambeaux étaient assez grands pour couvrir des défects étendus. Le
pédicule vasculaire est long, avec un large arc de rotation et une variation anatomique
minimale. La morbidité du site donneur est acceptable.
BIBLIOGRAPHY
- Roberts A.H., Dickson W.A.: Fasciocutaneous flaps for burn
reconstruction: a report of 57 flaps. Brit. J. Plast. Surg., 41: 150, 1988.
- Nahai F., Hill H.L., Hister T.R.: Experiences with the
tensor fascia lata flap. Plast. Reconstr. Surg., 63: 788, 1979.
- Bostwick J., Hill H.L., Nahai F.: Repair of large soft
tissue defects of inguinal region and perineurn with myocutaneous or omental flaps. Plast.
Reconstr. Surg., 63: 186, 1979.
- Wang T., Whetzel T., Mathes S.J., Vasconez L.O.:
Fasciocutaneous flap for vaginal and perineal reconstruction. Plast. Reconstr. Surg., 80:
95-102, 1987.
- Hayashi A., Maruyama Y.: The use of the anteromedial
thigh fasciocutaneous flap in the reconstruction of the lower abdomen and inguinal region;
a report of two cases. Brit. J. Plast. Surg., 41: 6338, 1988.
- Turley C.B., Cutting P., Clarke J.A.: Medial
fasciocutaneous flap of thigh for release of post-bum groin contractures. Brit. J. Plast.
Surg., 44: 36-40, 1991.
- Maruyama Y., Ohnishi K., Takeuchi S.: The lateral thigh
fasciocutaneous flap in the repair of ischial and trochanteric defects. Brit. J. Plast.
Surg., 37: 103, 1984.
- Ayad H.M.: Anatomical aspects of the anterolateral thigh
flap. Egyp. J. Plast. Reconstr. Surg., 18: 97-9, 1994.
- Larson D.L., Abston S., Evans E.B., Dobrkovesky M., Linares
H.A.: Techniques for decreasing scar formation and contracture in burned patients. J.
Trauma, 11: 807, 197 1.
- Mathes S.J., Nabai F.: Classification of the vascular
anatomy of muscles: experimental and clinical correction. Plast. Reconstr. Surg., 63:
788, 1979.
- Budo L, Finucan T., Clarke L: The inner arm fasciocutaneous
flap. Plast. Reconstr. Surg., 73: 513, 1984.
- Hill H.L., Hester R., Nahai R: Covering large groin
defects with the tensor fascia lata myocutaneous flap. Brit. J. Plast. Surg., 32: 12,
1979.
- Gopinath K.S., Chandra Shekhar M., Kumar M.V., Sirkant
K.S.: Tensor fascia lata myocutaneous flaps to reconstruct skin defects after radial
inguinal lymphadenectomy. Brit. J. Plast. Surg., 41: 366, 1988.
- Ponten B.: The fasciocutaneous flap and its use in soft
tissue defects of the lower leg. Brit. J. Plast. Surg., 34: 215, 198 1.
| This paper was received on 18 January
1995. Address correspondence
to: Hashem Mohamed Ayad M.D., Assistant Professor of Plastic and Reconstructive Surgery,
Tanta Faculty of Medicine, Tanta University, Tanta, Egypt. |
|




