| Annals of
Burns and Fire Disasters - vol. IX - n. 1 - March 1996
EXTENSIVE BURN SCAR
CARCINOMA IN THE SCALP AND ITS TREATMENT WITH FREE FLAPS: THREE CASE
AcartOrk S., Dalay
C., Yavuz M, Irik G, Kesiktas E.
Department of Plastic
and Reconstructive Surgery and Burn Unit, (~ukurova University Medical Faculty, Balcali
Hospita
SUMMARY. The
malignant potential of an unstable burn scar is ever present. It may develop in the scalp
regio body, such as the lower and upper extremities and the prestemal region. This paper
presents three cases of extensi oping in an unstable burn scar. Deep extensive excision is
necessary for this kind of expansive turnoral invasion, and are not sufficient to
reconstruct the complex scalp defect. After extensive excision of the tumour, free
latissimus do (two cases) and free radial artery forearm flap (one case) were carried out
to reconstruct the excisional defect. It is sue transfer is a good choice in the
reconstruction of deep extensive scalp defects.
Introduction
Malignant degeneration in long-standing
bum scars is frequently seen in clinical observation. In particular, ulceration, which
will heal spontaneously with appropriate treatment, may occur in patients who suffered
burns in early childhood and have lived their lives with the burn scar. Malignant
transformation of unstable bum scars must however also be considered as their malignant
potential is always present. A malignant neoplasm can appear in the burn scar in the scalp
region' or other parts of the body, such as the lower' and upper' extremities and the
prestemal region.
The exact incidence and precise mechanism of the malignant degeneration of bum scars are
not known. The commonest histological type of burn scar carcinoma is squarnous cell
carcinoma Basal cell carcinoma is believed to occur when the bum is more superficial and
the hair follicles and sebaceous glands are intact.
Different reconstruction techniques have been described for repairing scalp defects
created by tumour excision. These techniques depend on the extent of the tumour. Local
rotation or transportation flaps are widely recommended and are particularly useful in
bringing hair-bearing skin to sites that require hair for aesthetic reasons The multiple
flap technique described by Orticocheall and Jurill and the pericranial flap described by
Fonsecall may not be sufficient to cover defects after excision of extensive tumours in
burn scars. Distance flaps, both tubed" and flat," may be required when the skin
is insufficient to cover major defects.
Free flaps transferred from a distance by means of microsurgical techniques are reliable
procedures for the coverage of major scalp defects. These flaps offer the great dvantage
of one-stage repair with rich vascularization providing abundant skin and subcut~ groin
flap," free thoracodorsal axillai artery flap, free latissimus do flap and free
inferior epigastri advocated for this purpose.
This paper presents three patients who had lived many years with a bum scar on the scalp,
aft r bum scar carcinoma during adolescence. Because of the wide expansion of the tumour
and infiltration to the cranium, extensive excisions were performed and the scalp d~fects
were repaired with free tissue transfers.
Case reports
Case 1
F.A., a 39-year-old female, had suffered during infancy a deep bum
in the parieto-occipital region, living a zone of instability in the central area or me
scar admission a tumoral mass developed in treated in another hospital with local
thickness skin graft (STSG). On admis sented a grey-brown cauliflower-like t to-occipital
region (Figs. la, b). Biop! tumour was a squamous cell carcinon palpable adenopathy
in the left cervica indicated erosion and destruction of th( ded to perform a wide
excision of the cred during infancy n, leaving a zone of Six months before the scar which
was excision and splition the patient preumour in the pariey revealed that the a. The
patient had area. Radiography cranium. We deciscalp and cranium, with the aid of a
neurosurgeon, and t ? use a free flap for coverage. Following wide excision the scalp
defect measured 10 x 14 cm, with a cranium defec of 8 x 10 cm and a dural defect of 5 x 5
cm (Fig. ]c).
 |
 |
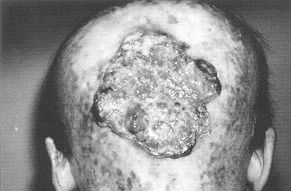
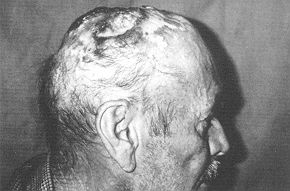
| Fig.
la - Recurrent and advanced squamous cell carcinoma on burn scar, occipital area;
posterior view. |
Fig.
1b - Recurrent and advanced squarnous cell carcinoma on burn scar, occipital
area; lateral view. |
 |
 |
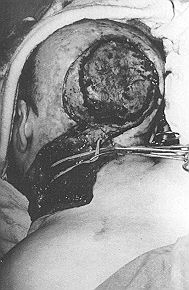
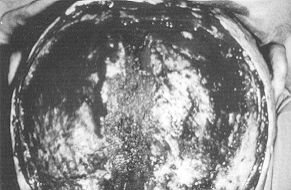
| Fig.
1c - Large excision of tumoral tissue and cra lymph node dissection performed and
recipient arter: for microanastomosis. |
Fig.
1d - Left latissimus dorsi myocutaneous flap prepared with long vascular pedicle.
|
 |
 |
| Fig.
le - Latissimus dorsi myocutaneous flap su and microvascular anastomosis
completed. Donor area mostly primarily. Split-thickness skin graft in only a small area |
Fig.
1f - Flap and split-thickness skin graft on tenth day after flap operation |
|
modified cervical lymph
node dissection, a left free latissimus dorsi (LD) myocutaneous flap was prepared, as
described by Maxwell et al." (Fig. Id). The LD myocuta neous flap was sutured
to the parieto-occipital area. End to-end arterial microvascular anastomis was performed
on the external carotid artery just after the facial branch and the thoracodorsal vein was
sutured end-to-( nal jugular vein. On removal of the micro the flap immediately became
full and pink. excessive tension of the distal suture line, sutures were removed on
distal skin edges, replaced on the LD muscle in the distal at The donor area was mostly
sutured primar area measuring 6 x 8 cm was covered " post-operative course was
uneventful.
Case 2
A.B., a 55-year-old male, had suffefed head burns during
childhood. Five years ago the scar became unstable and there was a non-healing wound in
the frontoparietal region. STSG was applied after excision ~f this area. On admission the
patient presented ulceration mass in the parietal region (Fig. 2a). Ther~ ble
regional adenopathy. Radiography showed erosion and destruction of the cranium in this area. A biopsy
revealed the tumour to be a basal cell carcinoma. Following extensive excision the scalp
defect in the parietal area measured 8 x 12 em and the cranium defect 7 x 11 ern (Fig.
2b). There was no dura defect. We decided to use a free radial artery (RA) forearm
flap from the patient's right forearm. This flap was prepared as described by Soutar et
al.' (Fig. 2c). The free forearm flap was sutured to the open area in order to
cover the defect (Fig. 2d). The superficial temporal artery was too thin and its
diameter too small and we considered that its arterial blood flow would not be sufficient
to nourish the forearm flap. The radial artery of the flap was therefore anastomosed to
the external carotid artery using a 6 em vena interposition. Two vein microanastomoses
were performed: vena comitans to the facial vein, and the subcutaneous vein of the flap to
the external jugular vein. On removal of all clamps, the free forearm flap immediately
became full and pink. MG was applied to the donor defect. The post-operative course was
uneventful and there were no post-operative flap or donor area complications (Figs. 2e,
f).
 |
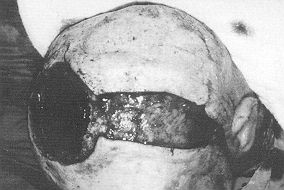 |
| Fig.
2a - Basal cell carcinoma in parietal region. |
Fig.
2b - Excision of tumour and cranium. |
 |
 |
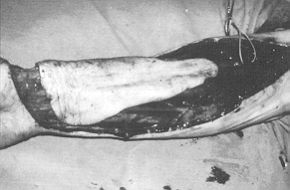
| Fig.
2c - Radial artery forearm free flap prepared and ready for transfer. |
Fig.
2d - Radial artery flap on parietal region. |
 |
Fig.
2e - Two weeks after flap operation. |
|
Case 3
H.C.. a 60-year-old male, had su the bilateral parietal area in infancy scar in this area.
On admission he pres tumoral lesions. Biopsy in the area in cell carcinoma in the scalp (Figs.
3a, b pable regional adenopathy. Radiogragraphy showed erosion and destruction of the
parietal cramu excision the scalp defect measured 14 the cranium defect 12 x 12 em and t
em. The dura defect was repaired wit the fascia lata. It was decided to cov free LD flap.
The LD flap was elevated pedicle with an 18 x 20 cm skin isla replacement of the LD
myocutaneo defect area, the thoracodorsal artery the left external carotid artery after it the vein to the external
jugular vein. were performed end-to-end. On removal of
all clamps the flap immediately
became full and pink (Figs. 3e, 1). The donor area was partly closed primarily and partly
with STSG in the area. During the post-operative course a partial flap necrosis developed
in the distal skin portion of the flap. The necrotic portion was excised, and STSG was
ured to the occipital area or area mostly sutured 11 area.
Discussion
Bum scar carcinoma occurs at an~
predilection." According to Nancarrm cer by definition has a latent period, (
induction mechanism may be added t producing neoplasia. There is an i between age at the
time of the orig latent period.' Burn scars on the exl scalp tend to be unstable. A scar
is when it corresponds to a zone of sm the slightest trauma can cause it to ulc ation
would therefore appear to be neoplasia.' Malignant transformation ble scars.
We present three cases of burr dating from childhood which had not developed into
neoplasia; there had been occasional episodes of ulceration, demonstrating the
characteristics of the unstable scar; malignant transformation was observed at later
stages. Case 2 is particularly interesting. Malignant transformation was not
observed in the unstable scar lesions which developed in the frontoparietal region and
were previously treated with STSG. This observation supports the protective role of the
grafting method.
In the cases we report, it was observed that tumoral tissue affected the cranium, and the
full layer of the cranium was excised. As the burn scar surrounded the tumour, local flaps
could not be performed. Local scalp flaps and pericranial flaps were not sufficient for
this particular of bum scar area.
In such cases free flaps are a good choice. Various free flap methods have been reported
for the closure of large scalp defects. McLean and Bunckell reported the first successful
coverage of the cranium by free tissue transfer using omental transplantation and
split-thickness grafting. Although omenturn can easily cover large defects of the head it
cannot provide durable cover, and laparotomy is required. Various flaps have been applied,
according to the characteristics of the individual case: free groin flap, free RA forearm
flap, free LD myocutaneous flap, and inferior epigastric flap.' If after excision the
defect is very large, the extensive flaps suggested by Batchelor and Sully may be used. A
large free tissue transfer was required for reconstruction. Cases requiring such a large
flap are however rare.
After excision of the tumour in the area covered by the burn scar, microvascular
anastomoses are performed in a distant area, so that well-vascularized tissue can be
transported. As a result well-vascularized tissue is transferred to a poorly vascularized
area. In our cases, the LD myocutaneous flap transferred to resurface the defects in
occipital and parieto-occipital regions was sufficient, length of the vascular pedicles
was adequat need to perform a vein interposition (Cases length of the vascular
pedicle is sufficien neck, and interpositional vein grafts are necessary. For the RA
forearm flap, the vasc long enough to reach the superficial temp( vein, if this artery and
vein are available. Otl graft is required to reach the neck vessels, Chicarilli et al.
were able to use the suped artery in all the cases presented in their paper.
In one of our patients (Case 1), in % formed scalp reconstruction by means of an
neous flap, the distal sutures were remov overcome excessive tension in the flap. In
Case 3 skin necrosis developed, including the distal myocutaneous flap. This
was excised and resurfaced by means of STSG. In our opini necrosis in this patient was due
to the flap's tation. Hardesty et al state that when larg muscle flaps are used in
vertically oriented defects, the weight of the flap, subjected to gravity, may pull the
flap away from the recipient inset suture line prior to flap adherence, and the tension at
the superior aspect of the wound caused by gravitational pull may result in local
ischaemia followed by necrosis of the suture line and thus partial flap loss and
separation.
The presence of clinically positive lymph glands at the time of presentation is very
important. One of our patients (Case 1) had palpable lymph nodes on admission and we
performed regional lymph dissection. In the other two cases there were no palpable lymph
nodes on admission and we did not perform lymphadenectomy. According to Nancarrow,' block
dissection should be reserved for clinically involved glands only. In the absence of
palpable node involvement, prophylactic node dissection is not necessary on a statistical
basis. The patient must however be observed at frequent intervals.
Microvascular free tissue transfer has a number of distinct advantages, including
avoidance of the size and reach limitations imposed by regional of one-stage
reconstruction without n procedures, essentially unrestricte( compared with local or
regional flap lity in designing and transferrin Microsurgery is not however without
cations, problems and risks.
 |
 |
| Fig.
3a - Extensive bum carcinoma on scalp a cranium with tumour. |
Fig.
3b - Extensive burn carcinoma on scalp and cranium with tumor. |
 |
 |
| Fig.
3c - The latissimus dorsi myocutaneous free flap with its long vascular pedicle. |
Fig.
3d - The latissimus dorsi myocutaneous free vascular pedicle. |
 |
 |
| Fig.
3e - Latissimus dorsi myocutaneous flap or parieto-occipital area microvascular
anastomosis performed in the left neck vessels. |
Fig.
3f - Latissimus dorsi myocutaneous fia microvascular anastomosis performed in the
left neck vessels. |
|
RESUME. La possibilitÕ du
dÕveloppement malin d'une cicatrice instable aprÒs br«lures est toujours prÕsente. Il
peut se rÕgion du cuir chevelu comme dans les autres rÕgions du corps, en particulier
les extrÕmitÕs supÕrieures et infÕrieures et nale. Les auteurs prÕsentent trois cas
d'une tumeur Õtendue du cuir chevelu qui s'est manifestÕe dans une cicatrice instable
faut effectuer une excision Õtendue et profonde dans ce type d'invasion tumorale
dilatable, et les lambeaux locaux ou rÕgio suffisants pour reconstruire ce dÕfaut
complexe du cuir chevelu. AprÒs l'excision Õtendue de la tumeur les auteurs ont appl
libre myocutanÕ latissimus dorsi (deux cas) et un lambeau libre de l'artÒre radiale de
l'avant-bras (un cas) pour reconstrui l'excision.
BIBLIOGRAPHY
- Casson P.R., Robins P.: Malignant
tumor of the skin. In: "Plastic Surgery" (ed. McCarthy), vol. 5, p. 3614. W.B.
Saunders Co.,Philadelphia, 1990.
- Horton C.E., Crawford H.H., Love
H.G., Leffler R.A.: The malignant potential of bum scar. Plast. Reconstr. Surg., 22: 348,
1958.
- Miyamoto Y., Harada K., Kodama Y.,
Takahashi H., Okano S.: Cranial coverage involving scalp, bone and dura using free
inferior epigastric flap. Br. J. Plast. Surg., 39: 483, 1986.
- Napoli B., D'Arpa N., Masellis M.:
Turnouts of the upper limb and burn scars. Case reports. Ann. Medit. Burns Club, 4: 251,
1991.
- Xie E., Li A., Wang S., Kang S.,
Cheng G.: Burn scar carcinoma: case reports and review of the literature. Ann. Medit.
Burns Club, 5: 102, 1992.
- Zermani R., Toschi S., Ricci R.: A
rare case of basal cell epithelioma. in a patient with burns sequelae. Ann. Medit. Burns
Club., 7: 218,1994.
- Castillo J., Goldsmith H.S.: Burn
scar carcinoma. Cancer J. Clin., 18:140, 1968.
- Nancarrow J.D.: Cicatricial cancer
in the South-West of England: a regional plastic surgery unit's experience over a 20-year
period. Br. J.Surg., 70: 205, 1983.
- Brown J.B., Fryer M.P.:
Reconstruction of electrical injuries including cranial losses with preliminary report of
cathode ray burns. Ann. 25.Surg., 146: 342, 1957.
- Kragh L.V., Erich J.B.: Treatment of
severe electrical injuries. Am. J. 26.Surg., 101: 419, 1961.
- Razemon J.P.: RÕparation des partes
de substance du cuir chevelu aprÒs br«lure. Ann. de Chir. Plast., 5: 187, 1960.
- Sinha JX., Khanna N.N., Tripathi
F.M., Bhattacharya V., Chowdhary M.D.: Electrical bums: a review of 80 cases. Burns, 4:
261, 1978.
- Orticochea M.: Four flap scalp
reconstruction techniques. Br. J. Plast.Surg., 20: 159, 1976.
- Juri J.: Use of parieto-occipital
flaps in the surgical treatment of baldness. Plast. Reconstr. Surg., 55:456, 1975,
- Fonseca J.L.S.: Use of pericranial
flap in scalp wounds with exposed bone. Plast. Reconstr. Surg.,72: 786, 1983.
- Bagozzi I.C.: Reparative procedure
in large losses of scalp and bone of the skull caused by serious electrical lesions. Br.
J. Plast, Surg., 8:49, 1955.
- Curtin JW., Latham W.D., Greeley
P.M., McNally R.E.: Catastrophic loss of scalp and contiguous structures. Plast. Reconstr.
Surg., 32: 1,1963.
- Chavoin J.P., Gigaud M., Clouet M.,
Laffitte F., Costagliola M.: The reconstruction of cranial defects involving scalp, bone
and dura fol lowing electrical injury: report of two cases treated by homograft free groin
flap and cranioplasty. Br. J. Plast. Surg., 33:311,1980.
- Baudet L, Guimberteau LC.,
Nascimento E.: S transfer of two free thoracodorsal axillary flaps. 58:680,1976.
- Chicarilli ZX, Ariyan S., Cuono
C.B.: Single-stage repair of comp ex sea p and cranial defects with the free radial
forearm flap. Plast. Reconstr. Surg., 77: 577, 1986.
- Earley M.J., Green M.F., Milling
A.P.: A critic use of free flaps in primary reconstruction of co calvarial cancer defects.
Br. J. Plast. Surg., 43: 283
- Jones N.F., Hardesty R.A., Swartz
W.M., Ramasastry S.S., Heckler cts of the scalp, middle third of the face and palate: the
role of mi rosurgical reconstruction. Plast. Reconstr. Surg., 82: 937, 1988.
- GUzel M.Z., Aydin Y., ~enyuva C.,
Aygit A.C~ Sanus Z., Mindikoglu AX, AltintaÏ M.: IlerlemiÏ rezeksiyonu sonucu oluÏan
geniÏ,skalp, kemik ve hemen onarimi iqin flep seqenekleriniD degerle Plast. Cerr. Derg.,
2: 188, 1994.
- Hardesty R.A., Jones N.F., Swarz
W.M., Ramasa F.D., Newton E.D., Schramm V.L.: Microsurgery microvascular free-tissue
transfer for massive dc and neck. Am. J. Surg., 154: 399, 1987.
- Maxwell G.B., Stueber K., Hoopes
J.E.: A frec myocutaneous flap. Plast. Reconstr., Surg. 62: 462 Soutar D.S., Sheker L.R.,
Tanner S.B., MacGrej forearm flap: a versatile method for intra-oral ree Plast. Surg., 36:
1, 1983.
This paper was
received on 20 March 1995.
Address correspondence to: Prof. Dr. Sabri AcartOrk,
Plastik ve RekonstrUktif Cerrahi ABD, Cukurov Universikey. tesi Tip FakUltesi, 01330
Balcali, Adana, Turkey
Tel.: +322.3386060/3226; Fax: +322.3386427 |
|