| Annals ofBurns and Fire Disasters - vol. IX - n. 2 - June 1996
AMNIOTIC MEMBRANES FOR TEMPORARY BURN COVERAGE
Hadjiiski 0., Anatassov N.
Burn and Plastic Surgery Centre, Pirogov Emergency Medical
Institute, Sofia, Bulgaria
SUMMARY. A survey is made of
the use of amniotic membrane as a temporary coverage for burn wounds. Amniotic membrane
can be used for superficial bums, deep burns, after necrectomy, on extensive granulating
wound surfaces, on autografts, in donor regions, and after dermoabrasion. Amniotic
membrane is readily available and does not present immunological problems. It does not
cause allergic responses and reduces water loss. The risk of the transmission of some
viral infections has to be taken into account. Bacterial examinations performed in 20
patients with burn wounds covered with amniotic membrane showed low or no bacterial
colonization of the burn surface. It is concluded that amniotic membrane should be more
widely used in this particular aspect of burn treatment.
The idea of using a biological dressing in
the treatment of extensive burn injuries has been increasingly put into practice in the
last 10 to 15 years. The two main reasons for its use are:
the increasing number of patients with
extensive deep burns who survive the acute period of trauma and require complex programmes
of plastic reconstructive treatment
the wide application of necrectomies
that leave raw areas of flesh requiring immediate post-operative coverage
Although the ideal temporary coverage has
yet to be found, those now available provide good possibilities for burn treatment.
Biological coverages should:
- be adherent to (and grow well on) the burn surface
- maintain low bacterial growth or prevent subsequent
bacterial contamination of the injured surface
- reduce the loss of fluids, microelements and proteins from
the injured surface
- have good fluid or gas permeability from the wound surface
towards the surrounding tissue
- be easy to handle, i.e. when placing on or removing from
the injured surface, and also fit closely to incised anatomical regions
- relieve pain, and promote care of the injury
- decrease the possibility of scar or keloid formation during
the healing process
- be available. in sufficient quantity and be reasonably
priced
Biological dressings have the following disadvantages:
- early graft rejection
- rapid, acute bacterial colonization of the injured area
There are three basic type of temporary
biological dressings available:
Biological skin dressings
- Allograft
- Xenograft: bovine, ovine, canine, porcine; cheap and
readily available; used fresh, frozen or lyophilized
- Cultured allograft: good results, but quite an expensive
method
- Collagen products: gel, sponges or other different plaques
- Amniotic membrane
Synthetic temporary skin dressings
These have many of the positive
characteristics of biological dressings, plus some other features (e.g. industrial
production, relatively low price), and include: Opsite, Omiderm and Duoderm.
Biosynthetic temporaryskin dressings
These are complex compounds of bioagents (collagen),
impregnated with silicone nets, such as Biobrane and Armigel. What is the role of amniotic
membrane in the topical treatment of burn injuries? Allo- and xenografts possess numerous
positive characteristics, but their use is sometimes limited, especially where tissue
banks have not been developed. Amniotic membrane has been used since 1912 with variable
success as a material for burn injury coverage. It has the following advantages:
- readily available in sufficient quantity
- application not associated with immunological problems
- large size
- simple to prepare and sterilize
- no allergic reactions
- up to 15% reduction of water losses in wounds
- histological structure similar to that of skin
The disadvantage of the use of amniotic
membrane is that there is some risk of viral infection transmission, e.g. hepatitis,
syphilis and AIDS.
Two varieties of amniotic membrane are mainly used:
- in toto (amnion + chorion) on deep burns
- amnion alone (epithelium + basic membrane) on superficial
burns
 |
 |
| Fig. la
- Superficial bum covered by amniotic membrane. Immediately after accident. |
Fig. 1b -
During treatment. |
 |
 |
| Fig. 1c - The
final result |
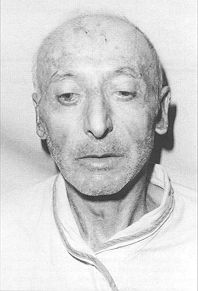
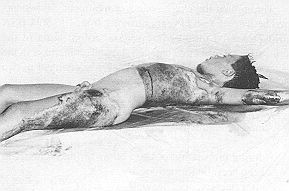
Fig. 2a - Nine-year-old
boy with deep bum. Immediately after accideni |
|
Indications for the use of amniotic membrane
Superficial burns
facial burns
limited superficial burns
open treatment of patients with large burn regions
Method of application: after
hospitalization of the patient, fresh burns are appropriately treated and the wound
surface is covered with amniotic membrane. A dry dressing is applied for 24 hours, which
makes the amniotic membrane adhere to the wound surface. The following day a control
dressing is performed, the membrane is changed if necessary, and if already dry, the burn
surface remains open until epithelialization is complete.
This method has some definite advantages: no painful dressing changes; no additional
bacterial contamination of wounds; reduction of fluid and protein losses from the bums.
The granulated burn presents a strong epithelium of good quality.
Throughout the entire course of treatment, 20 patients aged between 1 and 70 years
suffering from 1 to 50% 13SA burns presented little or no bacterial colonization of the
burn surface. Only three patients showed an increase in the bacterial microbial count; the
therapy was changed in two patients (Table I).
Deep burns
Amniotic membrane can be used:
- during preparation of deep burns for necrectomy, to keep
necrotic formations dry
- after necrectomies leaving raw areas of flesh - frequently
in combination with other temporary biological skin coverages and/or autografts
| BEFORE TREATMENT |
DURING TREATMENT |
1. St. epidertnidis +
St. aurcus 3. 101
KOE/cra2P |
St. aureti% 5. 1
WK0E/cin' |
2. Str.
(x-haemolyticus + St.
Epiderinidis 7.103 KOE/ern' |
N.B.G.
N.B.G. |
| 3. N.B.G. |
N.B.G. |
| 4. N.B.G. |
St. epidertnidis 2.
10' K 0 1 |
| 5. St. aureus 2. 10'
KOE/cin' |
3. 10' K |
6. St. epidermidis +
Enterococcu
6.10 KOE/cm' |
St. epidertnidis 5.
10' K 0 1 |
| 7. N.B.G. |
N.B.G. |
| 8. N.B.G. |
Saprophylic bacteria
<10 |
| 9. CiLrobacter sp. 3.
10' KOE/crn' |
N.B.G. |
| 10.
St.epideriiiidis+St.,tLti-eus6.101 |
N.B.G. |
| 11. St. epidermidis
10' KOE/ciW |
St. epidertnidis 2.10
KKOE/cm |
| 12. N.B.G. |
St. aureus 2. 10'
KOE/cm |
| 13. N.B.G. |
N.B.G. |
| 14.
St.epiderinidis9.10'KOE/cii)' |
St. epidertnidis 7.10
KOE/cm |
| 15. St. epidermidis 2.
10' KOE/cin' |
Ps. aureus 7.10 KOE/cm
|
16. Str.
f3-liaemolyticii.~, (A)T10'
KOE/crn' |
N.B.G. |
| 17. N.B.G. |
N.B.G. |
| 18. St. aureus 5. 10'
KOE/cin' |
St. aureus 7.10 KOE/cm
|
| 19. Saprophytic
bacteria 10' KOE/enV |
N.B.G. |
| 20.
E.coli,St.epidermdis4.10' |
St. epidertnidis 2.10
KOE/cm |
| |
N.B.G.: No bacterial growth |
|
| Table I - Bacterial flora before and during
the treatinent with amniotic membrane |
|
- on large granulating wound surfaces
- on widely perforated (1:3, IA) autografts
In some of these case, allo- or
xeno-grafts can be more effective, but if 1101 available they may he replaced by
amniotic membrane.
Compared with patients with superficial burns, in whom amniotic membrane dressing changes
are seldom necessary, patients with deep burns require more frequent changes, as the
dressings (end to disintegrate. However, the dressings always keep the underlying fiSSLIC
and viable, without any sign of local infection, and this helps to promote successful
autotransp ants.
Donor regions
These are immediately covered after graft
take and haemostasis; the amniotic membrane is left in place until complete
epithelialization of the donor region surface.
After dermoabrasion
The surgically prepared SUrfaCC is covered
with amniotic membrane, which detaches after healing ofthe abrasive SUffaCC.
Conclusion
- The positive features of amniotic membrane make it a
routine method of burn treatment.
- Despite more restricted indications for its use in
comparison with allo- or xenografts, amniotic membrane has a precise role in the treatment
of superficial and deep burns.
Amniotic membrane should be used more
intensively in burn treatment.
 |
 |
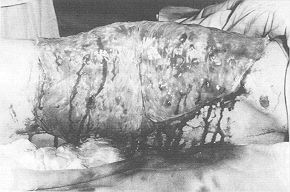
Fig.
2b - Wound surface covered with amniolic membrane after excision. |
Fig. 2c
- The final result. |
|
RESUME. Les auteurs
considèrent l'emploi de la membrane amniotique comme couverture provisoire des brûluics.
La nieintiranc ainniotique peut être usée pour les brûlures superficielles et
profondes, après la nécrectomie, sur les surfaces étendues (le lésions granuleuses,,
sur les autogreffes, dans les sites donneurs de peau, et après la dernioabrasion. La
membrane amniotique est facilement (li.,,Iionible et ne présente pas de problèmes
immunologiques. Elle ne cause pas de réactions allergiques et réduit les pcrte~
hydriqiics~. Il faut lenir compte (lu risque de la transmission de certaines infections
virales, Les examens, bactériologiques effectués dans 20 pa1i(,nl,,~ doit(
brûlur", étaient couvertes avec la membrane amniotique ont indiqué l'absence ou un
bas niveau de colonisation bactérienne (le, la surlace brûlée. Les auteurs concluent
qu'il faudrait employer plus diffusément la membrane amniotique pour cet aspect
particulier (lit traiteritent des brûlures.
BIBLIOGRAPHY
- Robson M.C. et al.: Amniotic membranes as a
temporary wound dressing. Surg. Gynecol. Obstet., 136: 904-6, 1973.
- Dioguardi D. et a].: Skin substitutes it) burn
treatment - our cxperience. Arm. Medit. Burns, Club, 3: 205 9, 1990.
- Atanassov N. et al.: The role of amniotic biological
dressings during burn wound management. Abstract Book of V1 National Conference on Burns
and Plastic Surgery, Bulgaria, 9- 10 Oct. 1992.
- Echinard C., Daniour 0., Combici R_ Saliabeddin L,
Vescovali C_ Dantzer E: Les biornatdriaux chei, lm, brCild.s Arm. Medit. Burns
Club, 4: 41-6, 1991.
- Echinard C., Latarjet J.: "Les br6lures",
Masson, Paris, 1993, p. 349.
- Hadjiiski 0., Atanassov N., Mzgalova J.: Biological
dressings in the management of burn wounds. Abstract Book of XXIX Congress of the European
Society for Surgical Researches, Montpellier, France, 16-19 May 1994. 7. Magliacani G.:
The surgical treatment of burns: skin substitutes. Ann. Medit. Burns Club, 3: 145-9, 1990.
- Quinby W.C., Hoover H.C., Schellan M. et al.:
Clinical trials of amniotic membranes in burn wound care. Plast. Reconstr. Surg., 70: 711,
1982.
Ramakrishnan K.M., Ruo D.T.:
Human amniotic membrane as a temporary biologic dressing in complicated burns in a
developing country. J. Burn Care Rehabil., 4: 202, 1983.
| This paper was received on 28 January
1995 Address correspondence to: Dr.
0. Hadjiiski, Center for Burns and Plastic Surgery, 21 Macedonia Blvd., Medical Institut
Pirogov, 1606 Sofia, Bulgaria. Tel.: 00.359.25153 - Fax: 00.359.2521717. |
G. WHITAKER
INTERNATIONAL BURNS PRIZE PALERMO (ITALY)
under the patronage of the Authorities of the Sicilian Region for 1997
By law n' 57 of June 14th 1983
the Sicilian Regional Assembly authorized the President of the Region to grant the
"Giuseppe Whitaker Foundation", a non-profit-making organization under the
patronage of the Accademia dei Lincei with seat in Palermo, an annual contribution for the
establishment of the "G. Whitaker International Burns Prize" aimed at
recognizing the activity of the most qualified experts from all countries in the field of
burns pathology and treatinent.
The amount of the prize is fixed at
twenty million Italian lire. The prize is awarded each year by the month ol'June in
Palermo at the seat of the G. Whitaker Foundation.
The Adjudicating Committee is
composed of the President of the Foundation, the President of the Sicilian Region, the
Representative of the Accademia dei Lincei within the G. Whitaker Foundation, the Dean of
the Faculty of Medicine and Surgery of Palermo University, three experts in the field of
prevention, pathology, therapy and functional re-covery of burns, the winner of the prize
awarded the previous year, and a legal expert nominated in agreement with the President of
the Sicilian Region as a guarantee of the respect for the scientific purposes which the
legislators intended when establishing the prize.
All persons who consider themselves
to be qualified to compete for the award are invited to send their detailed curriculum no
later than 31st January 1997 to Michele Masellis M.D., Secretary-Member ofthe Scientific
Cominittee, G. Whitaker Foundation, Via Dante 167, 90141 Palermo, Italy. |
|