| Annals ofBurns and Fire Disasters - vol. IX - n. 3 - September 1996
CENTRAL EMBOLIZATION BY A GUIDEWIRE IN A BURN PATIENT
Valero J.,(1) Barreiro J.,(1) S6ez E.(2) Vèzquez
Gonzalez (3) Lòpez-Suso E.,(1) Martelo F.(1)
(1) Burns Unit, Plastic Surgery Service, Juan
Canalejo Hospital, La Coruha, Spain
(2) Burns Unit, Anaesthesiology Service, Juan Canalejo Hospital
(3) Service of Cardiology, Juan Canalejo Hospital
SUMMARY. Few
risks are involved in the replacement of central venous catheters when guidewires are
used, but repeated practice, critical situations, and inexperience increase the
possibilities of error. A case is described in which a burn patient suffered embolization
of a guidewire during replacement of a central catheter. The situation was normalized
percutaneously using radiographic control without affecting the patient's later evolution.
Introduction
The use of central venous catheters in
burn patients is a widespread practice given the need for haemodynamic monitoring, the
administration of vasoactive drugs and large volumes of liquids, and, occasionally, total
parenteral nutrition. The risk of catheter infection in these patients is high, despite
the observation of aseptic measures during implantation and manipulation of the catheter,
and catheter replacement continues to be a routine practice. Replacing catheters using a
guidewire reduces the complications arising out of implantation but the technique is not
completely risk-free. In the case presented here, an entire guidewire was embolized in the
venous system during replacement of a catheter through the internal jugular vein. This is
an exceptional complication but it is possible that reports are not submitted because of
their iatrogenic origin.
Case report
A 53-year-old male with a daily
consumption of 40 cigarettes and more than 120 gm of ethanol who had suffered repeated
bouts of convulsive crises and delirium tremens fell on to a low flame while in a state of
severe alcoholic intoxication, suffering smoke inhalation and fullthickness burns in the
buttocks, scrotum, legs, and hands, involving 12% TBSA. The patient was transferred to our
Burns Unit where on admission, six hours after the accident occurred, he presented
oliguria/anuria and smokeinhalation symptoms, i.e. profound perioral and perinasal burns,
remains of soot in the oral cavity, and burned nasal vibrissae. A tube was inserted
orotracheally and the right internal jugular vein was accessed with the introduction of a
three-way catheter for perfusion. of lactated Ringer's solution, achieving haemodynamic
stability and recovery of renal function. Decompressive incisions were effected on the
hands and buttocks on admission, followed by fibre bronchoscoPy 24 hours post-admission
which confirmed the airway damage. Over the next few days, the patient developed
respiratory insufficiency and required mechanical ventilation. He also developed
intolerance to enteral nutrition, and total parenteral nutrition was initiated. on the
third day, the jugular catheter was changed using a guidewire, but during the replacement
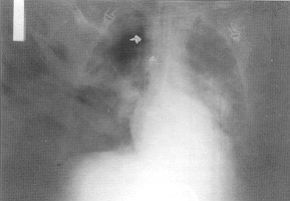
manoeuvre the guidewire was lost in the venous system. It was located radiologically and
seen to extend from the right subelavian vein to the iliac fork (Fig. 1). The patient was
immediately transferred to the haemodynamics ward where the guidewire was extracted
percutaneously through the left femoral vein using a loop-type 8F catheter under
radiological control ' On day 6 after admission, the burn area was slit and skin was
grafted. It was necessary to amputate the left leg and the 2nd, 3rd and 4th fingers of the
right hand.
 |
 |
| Fig. 1 - Guidewire pointed by
arrows in the RX thorax. |
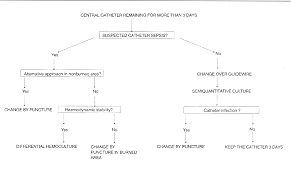
Fig. 2 - Management of central
venous catheter in a Burn Unit |
|
Before surgery, the right femoral artery
was accessed and the catheter located in the right internal jugular vein was replaced by
another in the left internal jugular for the purpose of monitoring during surgery. The
patient subsequently presented high fever and low blood pressure, leading to a diagnosis
of pneumonia at the base of the left lung. The central venous catheter was replaced by a
Swan-Ganz catheter, with haemodynamic support being initiated using vasoactive amines
(dopamine, dobutamine, and norepinephrine). Samples of blood and urine and bronchial
sweepings by telescopy and from the catheter tip were taken for cultures, and empirical
antibiotic treatment was initiated with the association of ceftazidime and vancomycin. The
bronchial sweepings were positive with growth of multiresistant Pseudomonas aeruginosa and
the initial antibiotic treatment was replaced by imipinem and amikacin. Death ensued
thirty days after admission due to multiple organ failure and sepsis.
Discussion
In burns units as in other intensive
care units, risk situations can arise out of human error. The patient in the case reported
here required the insertion of several central venous catheters in order to administer
vasoactive drugs, total parenteral nutrition and liquids and to monitor haemodynamic
function and gasometric values.
The use of venous catheters is associated with numerous mechanical complications, e.g.
unnoticed arterial puncture and catheterization,cervical bruising, haemothorax or
pneumothorax, cardiac perforation due to inappropriate location of the central venous
catheters, damage to the valve walls,' and arrhythmia, as also with infectious
complications, e.g. infection of the catheter tip and related sepsis, suppurating
thrombophlebitis, and endocarditis.
Although catheter change is not indicated in other groups -of patients unless there is
evidence of related problems," it is routine practice in the case of burn patients.
This practice is due to the high incidence of infection caused by the catheter and the
presence of suppurating thrombophlebitis,11 to the difficulty of making an early diagnosis
because of the almost invariable presence in extensively burned patients of a systemic
inflammatory response syndrome, and to the frequent presence of other foci of infection,
which makes diagnosis even more difficult. In the Burns Unit of the Juan Canalejo
Hospital, in order to reduce the risk of puncturing, replacement of the catheter is
carried out using a guidewire whenever there is a low degree of suspected infection and
the tip of the extracted catheter is sent for microbiological analysis. If the
semiquantitative culture is positive,` the replacement catheter is removed and a new
venous access point is obtained through puncture in another site. Only in the case of
severe limitations on venous access due to the presence of burns in the puncture area is a
haemoculture technique applied through the suspected catheter, together with haemoculture
of a blood sample taken from a peripheral vein.
Replacing catheters using guidewires is easy and cheap, and reduces the mechanical risks
derived from punctures, without increasing risks of an infectious nature.',' Nonetheless,
as shown by the case history reported here, the technique is not entirely risk-free. In
addition to the possibility of losing the whole guidewire, one must also consider the
embolization of fragments which may easily reach the pulmonary artery. The extraction of
such fragments, even using radiographic control techniques, is difficult and occasionally
thoracic surgery is required, although the risks deriving from the patient's general
condition may necessitate postponement of the operation. Embolization of fragments is
generally caused by unnoticed severing of the catheter during implantation, although this
may also occur during withdrawal; embolization is also possible in central and peripheral
catheters. Embolization of the entire guidewire is due to lack of practice in use of the
technique or to situations of haemodynamic instability in a patient with poor alternative
venous access, leading to errors caused by the need for rapid replacement of the catheter.
In conclusion, although replacement of a catheter using a guidewire reduces the risk
factor, the procedure must be carried out by expert personnel and a separate venous access
of good quality should be maintained, even if only temporarily, in order to avoid errors
due to inexperience or to situations of stress in the medical staff performing the
technique.
RESUME. La procédure du remplacement des
cathéters veineux centraux ne présente pas de risques si l'on use des fils de guide,
mais la répétition continue, les situations critiques, et l'inexpérience peuvent
augmenter les possibilités d'erreur. Les Auteurs décrivent le cas d'un brûlé qui a
souffert l'embolisation d'un fil de guide pendant le remplacement d'un cathéter central.
La situation a été normalisée par voie percutanée en employant un contrôle
radiographique, sans effets pour le décours successif du patient.
BIBLIOGRAPHY
- Peres P.W.: Positioning central venous catheters. A
prospective survey. Anaesth. Intens. Care, 18: 536-9, 1990.
- Oishi A.J., Zietlow S.P., Sarr M.G.: Erroneous
arterial placement of a central venous catheter. Mayo Clin. Proc., 69: 287-8, 1994.
- Rider M.A., Chell J.: latrogenic haematoma causing
airway obstruction in a burned patient. Bums, 20: 260-1, 1994.
- Hagley M.T., Martin B., Gast P., Traeger S.M.:
Infectious and mechanical complications of central venous catheters placed by percutaneous
venipuncture and over guidewires. Crit. Care Med., 20: 1426-30, 1992.
- Senagore A., Waller J.D,, Bonnell B.W, Bursch L.R.,
Scholten D.J.: Pulmonary artery catheterization: a prospective study of internal jugular
and suliclavian approaches. Crit. Care Med., 15: 35-7, 1987.
- Scott W.L.: Complications associated with central
venous catheters. A survey. Chest, 94: 1221-4, 1988.
- Elliot C.G., Zimmerman G.A., Clemmer T.P.:
Complications of pulmonary artery catheterization in the care of critically ill patients.
A prospective study. Chest, 76: 647-52, 1979.
- Boyd K.D., Thomas S.J., Gold J., Boyd A.D.: A
prospective study of complications of pulmonary artery catheterization in 500 consecutive
patients. Chest, 84: 245-9, 1983.
- Pinilla J., Ross D.F., Martin T., Crump H.: Study of
the incidence of intravascular catheter infection and associated septicemia in critically
ill patients. Crit. Care Med., It: 21-5, 1983.
- Strinden W.D., Helgerson R.B., Maki D.G.: Candida
septic thrombosis of the great central veins associated with central catheters. Ann.
Surg., 202: 653-8, 1985.
- Greerie J.F., Fitzwater J.E., Clemmer T.P.: Septic
endocarditis and indwelling pulmonary artery catheters. JAMA, 233: 891-2, 1975.
- Savage A.P., Picard M., Hopkins C.C., Malt R.A.:
Complications and survival of multilumen central venous catheters used for parenteral
nutrition. Br. J. Surg., 80: 1287-90, 1993.
- Pruitt B.A., McManus W.F., Kim S.H., Treat R.C.:
Diagnosis and treatment of cannula-related intravenous sepsis in burn patients. Ann.
Surg., 191: 546-60, 1980.
- Maki D.G., Weise C.E., Sarafin H.W.: A
semiquantitative culture method for identifying intravenous -catheter-related infection.
N. Engl. J. Med., 296: 1305-9, 1977.
- Richardson J.D., Grover F.L., Trinkle J.K.:
Intravenous catheter emboli. Experience with twenty cases and collective review. Am. J.
Surg., 128: 722-7, 1974.
- Polos P.G., Sahn S.A.: Complication of central
venous catheter insertion: Fragmentation of a guidewire with pulmonary artery embolism.
Crit. Care Med., 19: 438-40, 1991.
Reynen K.R.: 14-year follow-up of
central embolization by a guide wire. N. Engl. J. Med., 329: 670-1, 1993.
This paper was
received on 23 March 1996.
Address correspondence to: Dr J. Valero, Burns
Unit, Plastic Surgery Service, Juan Canalejo Hospital, La Corufla, Spain. |
|