| Annals of Burns and Fire Disasters - vol. IX - n. 3 - September
1996
SEVERE COMPLICATIONS IN ELECTRICAL BURNS (INCLUDING
VISCERAL COMPLICATIONS)
Haberal M.,(1,2) UQar K.(1), Bayraktar
0.(2), Oner R .(2).
(1)Baskent University, Ankara Hospital, Ankara,
Turkey
(2)Burn Unit, Hacettepe University Hospital, Ankara
SUMMARY. Over
a period of 13 years (1979-92), 1065 patients were admitted to the Bum Unit at the
Hacettepe University Hospital, Ankara. Of these, 219 (20.1%) suffered from electrical
injury. The patients were treated according to a routine protocol. The most important
early complications were acute renal failure, sepsis, and associated skeletal and central
nervous system injuries. The late complications were total or partial extremity
amputation, scars and contractures, cataract, and epilepsy. The mortality rate was 21.5%
(47 patients, of whom 26 died of multiple organ failure, 13 of sepsis, and 8 of severe
cerebral trauma). The high overall incidence and rate of severe cornplications in
electrical burns compared with those found in other reports show that electrical injury
still constitutes a life-threatening problem in our country. The victims often suffer the
physical and psychological consequences of late complications, such as amputation. To
prevent these undesired effects, preventive measures are urgently required through a
massive education campaign, together with the realization and maintenance of high
industrial safety standards.
Introduction
Electrical injuries constitute a
relatively large proportion of burns in Turkey. According to our previous epide-
miological studies, as niany as 20% of the bums treated in our bum unit were caused by
electricity. 1,2 Severe complications, including injuries to the visceral organs and
amputation in the four extremities, were not infrequent in our series.' This study was
performed to investigate the overall complications caused by electrical burns treated in
our centre.
Patients and methods
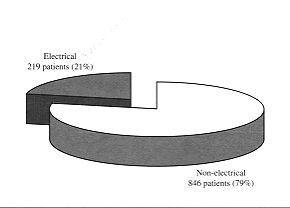
Between 1979 and 1992, 1065 patients
were admitted to the Burn Unit at the Hacettepe University Hospital, Ankara. Of these, 219
(20.1%) presented electrical injury (Fig. 1). The male to female ratio was 9.3A.
|
Fig. 1 -
Distribution of patients with electrical and non-electrical burns. |
|
The majority of the patients were young
dult males but there were also 67 children (30. 1 %) under the age of 15 yr, of whom
twelve (17.9%) were aged between 0 and 6 yr and 55 (82.1%) between 7 and 15 yr (Fig. 2).
The most frequent causes of the accidents were carelessness, the employment of young
persons without occup ' ational education, negligence by the electrical company, lack of
parental supervision, and mischievous behaviour. The patients were treated according to a
routine protocol. Following fluid and electrolyte resuscitation, all the systems were
examined to detect any associated injury due to electricity, including stroke. Emergency
dialysis was performed when massive myoglobulinuria and acute renal failure were bserved.
Necrotic tissues were usually debrided sequentially in order to preserve any salvageable
part. The topical agents preferred were polyvidone iodine and silver sulphadiazine.
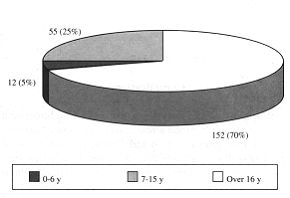 |
Fig. 2 -
Distribution by age of patients with electrical burns. |
|
Wound closure was effected with flaps or skin grafts., as
needed. The physical, psychological and social rehabilitation of the patients was provided
during and after hospitalization.
Results
The severe complications noted in this series are
summarized in Table 1.
| Complications |
Patients |
| N |
% |
| Musculoskeletal |
62 |
28.3% |
| Extremity amputation |
56 |
25.6% |
| One extremity |
33 |
15.1% |
| Two extremities |
16 |
7.3% |
| Three extremities |
6 |
2.7% |
| Four extremities |
1 |
0.5% |
| Rib fracture |
3 |
1.4% |
| Bilateral femur fracture |
1 |
0.5% |
| Metatarsal bone fracture |
1 |
0.5% |
| T3-T4 fracture |
1 |
0.5% |
| Neurological |
44 |
20.1% |
| Central nervous system |
38 |
17.4% |
| Haemorrhage |
18 |
8.2% |
| Neurophysiological disturbance |
18 |
8.2% |
| Transient anisocori a |
1 |
0.5% |
| Persistent epilepsy |
1 |
0.5% |
| Peripheral nervous system |
6 |
2.7% |
| Severe impairment of hand |
|
|
| function due to nerve injuries |
6 |
2.7% |
| Cardiac |
4 |
1.8% |
| Myocardial infarction |
1 |
0.5% |
| Supraventricular tachycardia |
3 |
1.4% |
| Renal |
32 |
14.6% |
| Acute renal failure |
32 |
14.6% |
| Septic |
146 |
66.7% |
| Visceral |
4 |
2.7% |
| Massive small bowel necrosis |
1 |
0.5% |
| Stomach perforation |
1 |
0.5% |
| Colon necrosis |
1 |
0.5% |
| Pleural injury and lung contusion% |
1 |
0.5% |
| Gastrointestinal bleeding |
2 |
0.9% |
| Ocular |
4 |
1.8% |
| Keratoconjunctivitis |
2 |
0.9% |
| Cataract |
2 |
0.9% |
|
| Table 1 - Complications in electrical bums |
|
Complications
Musculoskeletal: Fifty-six
patients (25.6%) underwent at least one partial or total amputation of the injured
extremities. Of these patients, 16, 6 and 1 required total or partial amputation of
respectively two, three and four extremities. Rib fractures were found in three patients.
Bilateral femur fracture was observed in one patient, metatarsal bone fracture in another,
and there were three fractures of cranial bones. One patient had paraplegia due to T3-T4
fracture.
Neurological: Thirty-five patients fell following a stroke and eight of the 18
patients with severe cerebral complications (haemorrhage) died. Eighteen patients
developed various neurophysiological complications due to electrical injury to the brain.
Disorientation was common in these patients. One patient had transient anisocoria, and one
became epileptic. Six patients suffered severe impairment of hand function due to
neuromuscular destruction by the electric current. Two of these underwent free
neurovascular gracilis musculocutancous flap transfer to substitute flexors of the hand.
Cardiac: Important electrocardiographic alterations were present in four patients
(non-specific ST-T waves and sinus tachycardia were not considered). Three of these had
supraventricular tachycardia, while the fourth showed evidence of inferior myocardial
ischaernia, which had not been recorded prior to the electrical injury.
Renal: Thirty-two patients (14.6%) presented acute renal failure. Of these, twenty
required peritoneal dialysis or haemodialysis (Table II).The mean delay in arrival
time in these patients was 3.5 days. Only two patients arrived on the day of the accident.
Some patients were sent to our burn unit for haemodialysis. Most of these patients had not
received appropriate fluid and electrolyte therapy during transportation or at the
previous hospital. Seven patients died, despite vigorous fluid and electrolyte
resuscitation and dialysis.
Visceral: Four patients had visceral injuries involving thoracic or abdominal
organs. One of these patients was a 36-year-old male electrician, who was brought to our
hospital the day after an electrical injury in the abdomen. He had received inappropriate
resuscitation. Following emergency resuscitation ptocedures, he underwent massive small
bowel resection but died the following day of multiple organ failure. The second patient
was a 15-year-old male with electrical injuries in the abdomen and the lower extremities.
After surgery for stomach perforation and amputation of both legs, he developed a
high-output intestinocutaneous fistula. Hyperalimentation was initiated but the patient
died 40 days post- operatively owing to sepsis. The third patient had colostomy, which was
subsequently closed. The fourth patient was subjected to thoracotomy and resection of the
third and fourth ribs. A thoracic tube was applied and the patient was discharged after
two months. Two patients had gastrointestinal bleeding.
Ocular: Two patients with keratoconjunctivitis were attended by ophthalmologists. Cataract
developed in two patients several months following discharge. Both patients underwent lens
extraction.
| |
Peritoneal
dialysis |
Haemodialysis |
Both |
None |
Total |
| Alive |
4 |
3 |
2 |
6 |
15 |
| Deceased |
9 |
1 |
1 |
6 |
17 |
| Total |
13 |
4 |
3 |
12 |
32 |
|
| Table II - Number of patients with renal failure |
|
Mortality
The mortality rate was 21.5% (47 patients). Twentysix
of these (55.3%) died of multiple organ failure. In thirteen patients (27.7%) the cause of
death was sepsis, and in eight (17.0%) severe cerebral trauma.
Discussion
The high overall incidence and rate of
severe complications in electrical burns compared with those reported in other countries
show that electrical injury still constitutes a life-threatening problem in Turkey.
Musculoskeletal complications constituted one of the major complication groups in our
series. However, the high amputation rate (37.4%) in our previous series in 1985 declined
to 25.6% in the present study. This may be due to earlier decompression and debridement of
the injured extremities in recent years .6 This rate is consistent with reports from other
countries .
A decrease from 18.1 % to 14.6% was also noted in the rate of renal failure compared with
our previous series.',' This may be correlated to the early administration of fluid and
electrolyte resuscitation during transportation. This rate was however higher than that
reported in other series (15-7.5 %).4, ' The mean delay in arrival time from a
nonspecialized facility to our unit of patients suffering from severe renal insufficiency
was 3.5 days. Although these patients were subjected to extensive haemodialysis and
peritoneal dialysis, no improvement could be obtained.
Neurological complications occurred in two ways, either by direct electrical trauma or by
a fall from a height, resulting sometimes in severe intracranial haemorrhage and death.
The mortality rate with this complication was hirgh in the present
series.Neurophysiological disorders were also common. One patient presented persistent
epilepsy. Severe peripheral nerve disorders were also not uncommon. One patient became
paraplegic as a result of T3-T4 fracture.
Cardiac complications were rarely observed, contrary to theoretical expectations. Only one
patient developed myocardial infarction and none died of cardiac complications.
Septic complications were consistent with those in other series.' The mortality rate due
to sepsis was however higher. This may be attributed to the late arrival of patients who
had already become septic in a non-specialized facility and received inappropriate
treatment.
Although not frequent, visceral injuries may be encountered following electrical injury in
the thoracic and abdominal walls.' In the present series four cases were reported. Two
patients died from this type of injury. It is essential to operate on patients with
abdominal or thoracic electrical injuries as soon as possible. In the present series and
in those of other authors, death was inevitable when surgery was delayed.
Ocular complications were also noted, but not frequently. Two patients (1.8%) developed
cataract.
The present study reflects the importance of electrical burns in our country. The victims
often suffered the physical and psychological consequences of late complications, such as
amputation. To avoid these unwelcome circumstances, preventive measures are urgently
required, with wide-ranging education campaigns and the achievement and perfection of
industrial standards.
RESUME. Pendant une période
de 13 ans (1979-1992), 1065 patients ont été hospitalisés dans l'Unité de Brûlures de
l'Hôpital Universitaire Hacettepe, Ankara. De ces patients 219 (20, 1 %) souffraient de
lésions électriques. Les patients ont été traités selon un protocole de routine. Les
plus importantes complications précoces étaient l'insuffisance rénale aiguë, la
sepsis, et les lésions associées squelettiques et du système nerveux central. Les
complications tardives incluaient l'amputation totale ou partielle des extrémités, les
cicatrices et les contractures, la cataracte, et l'épilepsie. Le taux de mortalité
était 21,5% (47 patients, dont 26 pour insuffisance organique multiple, 13 pour sepsis,
et 8 pour trauma cérébral sévère). Le haut niveau de l'incidence et du taux des
complications sévères des brûlures électriques par rapport à celui observé par
d'autres chercheurs indique que les lésions électriques continuent à représenter un
danger mortal dans notre pays. Souvent les victimes souffrent des conséquences physiques
et psychologiques pour les complications tardives, comme l'amputation. Pour éviter ces
effets malheureux il faut appliquer des mesures de prévention à travers une campagne
massive d'éducation, et dans le même temps réaliser et maintenir un niveau élevé des
standards de sécurité industrielle.
BIBLIOGRAPHY
- Haberal M.: Electrical bums: a five-year
experience - 1985 Evans Lecture. J. Trauma, 26: 103, 1986. Haberal M., Ugar N., Bayraktar
C., Oner Z.: Analysis of 1005 bum patients treated in our centre. Ann. Medit. Bums Club,
6: 73, 1993.
- Haberal M., Oner Z., Gfilay H. et al.: Severe
electrical injury and rehabilitation. Ann. Medit. Bums Club, 1: 121, 1988.
- Hanumadass M.L., Voora S.B. et al.: Acute electrical
bums: a tenyear clinical experience. Burns, 12: 427, 1986.
- Gordon M.W., Reid W.H., Awwaad A.M.: Electrical
burns - incidence and prognosis in Western Scotland. Bums, 12: 254, 1986.
- Holliman C.J., Saffle J.R., Kravitz M. et al.: Early
surgical decompression in the management of electrical injuries. Am. J. Surg., 1:13,1982.
- Haberal M., Yilmaz E., Oner Z.: Renal complications
in electrical bums. Bull. Clin. Rev. Burn Injury, 1: 37, 1984.
- Wilkinson C., Wood M.: High voltage electric injury.
Am. J. Surg.,136:693,1978.
- Luce E.A., Gottlieb S.E.: "True" high
tension electrical injuries. Ann. Plast. Surg., 12: 321, 1984.
| This paper was received on 26
September 1994. Address
correspondence to: Prof. M. Haberal, FACS, 1 Cadde No. 77 Kat 4, Ankara, Turkey. |
AWARD OF THE G.
WHITAKER INTERNATIONAL BURNS PRIZE PALERMO, ITALY
FOR 1996
The official prize-giving was
held on September 26th 1996 in Palermo at the seat of the G. Whitaker Foundation in the
presence of the, authorities and of representatives of the academic, scientific and
cultural world.
The 1996 prize was awarded to Prof.
John Burke, M.D., Emeritus Professor of Surgery at the Harvard University Medical Faculty
and Emeritus Director of the Trauma Service, Massachussetts General Hospital, Boston USA.
The Prize was awarded with the following
motivation:
"for dedicating a lifetime to
teaching and to assistance of patients in the sector of surgery. He has a vast and
qualified activity in the field of burns, to the knowledge of which he has contributed
with numerous publications on various aspects, in particular infection and metabolism. His
studies for the realization of artificial skin and the use of biomaterials have been
notable". |
|