| Annals of'Burns and Fire Disasters - vol. IX - n. 3 - September
1996
THE TREATMENT OF ELECTRICAL BURNS IN THE VOLAR PART OF THE ADIOCARPAL REGION Beiba GA. Clinic of Plastic Surgery and Burns, U.C.H.T, Tirana, Albania SUMMARY. In electrical bums in the volar part of the radiocarpal region, with damage to the u1nar and radial arteries, it is of great importance to preserve the posterior interosseous artery. It is this artery, together with the dorsal carpal arch and other anastomoses, that ensures vascularization of the hand. A regional anatomical description is given in relation to different stages of the surgical protocol. An evaluation is made of early necrectomy, decompression of the muscle compartment, ligation of damaged vasal stumps, surgical re-exploration, and the closure of wounds with skin grafts. The treatment of electrical trauma in this region of the body is debated on the basis of the description of a number of cases. Introduction Electrical injuries in the radiocarpal
region create many problems for both patient and surgeon. The involvement of various
anatomical structures and the depth of the lesions not only jeopardize hand function but
often raise the question whether to preserve the hand or not. The decision of the surgical
staff is a constant source of debate, but if the question were clearly put - i.e.,
"will the patient accept in this first phase of treatment the hand without function
or a prosthesis?" - the discussion could be more rapidly concluded. In fact all our
patients have preferred the first alternative. In consultations with them and their
families, we have noted that there is usually a strong desire to preserve the hand, even
if only for external appearance. This logic seems to be justified, as nobody can readily
accept the trauma of amputation of the hand, since it is natural to hope for functional
improvement at a later stage. Clinical material In the period 1992-1993 we treated
eight cases of electrical bums in the radiocarpal region. In three of the cases, in view
of the deep tissue destruction, we performed amputation in the upper part of the
antebrachial region. In the other five cases the electrical trauma was concentrated in the
volar part of the radiocarpal region, with damage to the two main arteries. In one of
these five cases the injury was located only in the radiocarpal region, while in the other
four the injury also affected other parts of the body (mean BSA, 11.5%). In these
five patients (all male, average age 22.4 yr) necrectomy was performed either on the day
of admission or the following day. complete necrectomy of all injured zones, muscular decompression, preservation of posterior interosseous arteries, ligation of damage vasal stumps exploration necrectomy of the radiocarpal region skin graft on the wounds, including the radiocarpal region In two patients, at the end of the operation, we used an autotransplant as a biological dressing, while in the third patient it was necessary to apply an osteosynthesis, as the radiocarpal articulation was open. On discharge, the patients had a consolidated transplant and vascularized but nonfunctioning hands, because of the injury to the nerves and the main flexor tendons. Only some slight extensor movement of the fingers was seen. The mean hospitalization period for the five patients was 63.3 days. At the last follow-up we did not observe any disturbances of the veDolymphatic circulation or the appearance of neurotrophic lesions. Discussion In the event of complete destruction
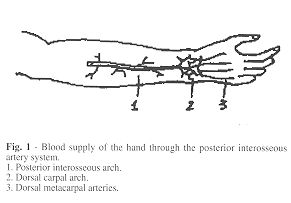
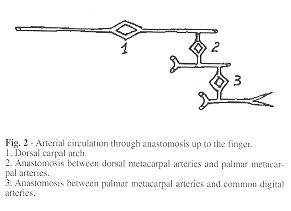
of the radial and ulnar arteries in volar electrical trauma in the radiocarpal region,
anatomical considerations suggest that it may be possible to vascularize the hand by means
of the interosscous system, and in particular through the posterior interosseous artery.
This artery is located in the posterior part of the forearm, and if not affected by the
electric current it assumes great importance for the maintenance of vascularization of the
hand through the dorsal carpal arch. It is an artery of considerable diaiiieter (0.9-2.7
mm)l and the blood flow through it is potent, also because the circulation of blood ceases
in the radial and ultiar arteries, while the blood flow is unchanged in the brachial
artery in the antecubital fossa.
The method of surgical treatment makes use of certain techniques whose function is to preserve vascularization of the hand. Immediate necrectomy accompanied by decompression of the muscular compartments',' has to be performed as soon as the patient's condition permits it. One aim of this procedure is to preserve the pronator quadratus muscle and, if this is not damaged, to stimulate carpal anastomosis of both interosseous arteries, and also to regulate the posterior interosseous circulation when this functions alone. Decompression in the posterior compartment of the forearm and the practising of small skin incisions are not justified, as these procedures would irreparably damage the vascularization of the hand. We are of the opinion that the preservation of the septocutaneous arteries in this region also contributes to hand vascularization. During the same surgical operation, we ligate the radial and ultiar arteries in order to prevent late acute haemorrhage.
As with all electrical burns, the surgeon
is right to perform new local explorations for the realization of full necrectomy, thus
creating conditions for quick granulation. Excision as far as the carpal bones, the
opening of articulations and the removal of a carpal bone can all be performed without
hesitation, when the indications are complete. Although we are working on a bony plane, we
have observed that granulation is not late - on the contrary, there may be
hypergranulation if covering is delayed. Finally, closure of the wound is performed with a
middle-thickness transplant. RESUME. UAuteur soutient l'importance, dans les brûlures électriques de la partie palmaire de la région radiocarpienne, avec des lésions dans les artères cubitale et radiale, de préserver l'artère interosseuse postérieure. Cette artère, avec le réseau artériel carpien dorsal et d'autres anastomoses, assure la vascularisation de la main. Après avoir décrit l'anatomie régionale par rapport aux phases successives du protocole chirurgical, l'Auteur évalue la nécrectomie précoce, la décompression du compartiment musculaire, la ligature des moignons vasculaires lésés, la réexploration chirurgicale, et la réparation des lésions avec des greffes cutanées. Enfin il considère le traitement des traumatismes électriques dans cette région du corps à la lumière de la description de divers cas. BIBLIOGRAPHY
|