| Annals ofBurns and Fire Disasters - vol. IX - n. 3 - September 1996
BURNS SEQUELAE IN CENTRAL AFRICA: REPORT ON THE TREATMENT
OF ELEVEN CASES
Gandini D.
Divisione di Chirurgia Plastica, Ospeclale di
Cisanello, Pisa, Italy
SUMMARY.
The results are presented of 11 cases of burn sequelae, mainly in children, treated by an
Italian team in the Zambian-Italian Hospital in Lusaka (central Africa). From a technical
point of view the surgical procedures do not present particular problems, but in the
social context of central Africa they assume great value because they not only improve the
quality of life of the unfortunate children but may become a sine qua non for their
survival. In Zambia, as in all central Africa, burns are not treated in any specific way.
The few surviving patients suffer from extremely severe scar contractures, with tragic
consequences. This paper describes the cases treated and the results obtained.
Introduction
Burns are frequent accidents in
central African rural areas. The routine use of fire for domestic needs and the flammable
materials used for the construction of huts are the main causes of burns. Zambia, like
most other countries in central Africa, lacks a specialized burns unit. Fluid replacement
therapies and infection prevention techniques are performed only occasionally and in very
few hospitals. Even basic treatment is difficult to administer in many instances - most
patients receive no therapy whatsover and the burns are left to heal spontaneously.
McCarthy' asserts that in primitive and archaic societies children with congenital
deformities are "often removed from the tribe or cultural unit and left to die in the
surrounding wilderness.
A similar attitude, although not so radical, can still be observed in central Africa with
regard to any kind of congenital and acquired handicap. Possibly also the fatalism of the
African way of thinking has a negative influence on this attitude. The quality of life for
a handicapped child in central Africa is extremely poor, and a severe scar contraclure can
easily become a tragedy. As a result mortality due to burns is very high, and even burns
of medium severity can result in very severe scar contracture. The burned child is doomed
to a tragic and desperate life without any social support except that offered by
humanitarian and religious organizations, which cannot however cover the whole country.
Consequently, simple routine surgical procedures can not only improve the quality of life
of these unfortunate children but sometimes become a sine qua non for their survival.
In summer 1995 1 had the privilege of serving as Junior Surgeon in an Interplast Team
(Senior Surgeon, Paolo Santoni-Rugiu, M.D., Ph.D.) in Zambia. In the hospital where our
team was working (Zambian-Italian Hospital for Handicapped Children, Lusaka; Chairman,
Prof. J.G. Jellis, FRCS) a great number of patients who suffered burn injuries in the past
were observed.
It may be of some interest to report on the rehabilitation of the cases of scar
contracture that 1 had the opportunity to treat, since such cases are rarely observed
nowadays in the western world.
Case reports
Eleven patients with severe post-burn
scar contractures were treated, of whom nine were aged between 6 and 10 years and the
other two respectively 16 and 48 years.All the children in this series showed signs of
nutritional deficiencies and lab tests showed constant severe anaemia (Hb less than 9).
Bum injury four years previously in right lower limb. Scar contracture with severe flexion
of right knee (45'); foot also flexed and adherent to anterior aspect of the leg (Fig. 1).
 |
 |
| Fig.
1 - Severe post-burn contracture of knee and ankle. |
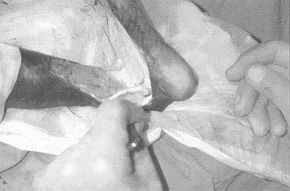
Fig.
2 - Scar incised on anterior aspect of ankle. Tendolysis performed. |
 |
 |
| Fig.
3 - Kirschner wire used to stabilize joint after tibiotarsal capsulotomy. |
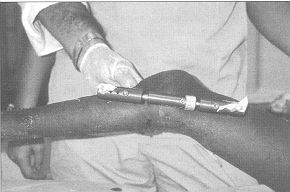
Fig.
4 - De Bastiani external device used to maintain and gradually increase extension
by daily adjustment of screw. |
 |
 |
| Fig.
5 - De Bastiani external device used to maintain and gradually increase extension
by daily adjustment of screw. |
Fig.
6 - Complete extension obtained within 35 days. External fixation device removed.
Patient initiates physiotherapy after 10 days. |
|
The patient was operated on in general
anaesthesia. The scar in the knee was relaxed with a Z-plasty. The extension was obtained
through elongation of all the flexor tendons, which was obtained by dividing them along
the axis, and capsulotomy of the knee. The flaps of the Z-plasty were insufficient to
cover all the raw area in the posterior aspect of the limb and two skin defects in the
thigh and leg had to be covered with a split skin graft.
The foot was mobilized by incising the scar anteriorly (Fig. 2). The tendon of the
long peroneal muscle was elongated by dividing it along the axis while the tendon of the
peroneal brevis was simply cut. A tibiotarsal capsulotomy completed the extension of the
foot.
The extension of the tibiotarsal joint was maintained with a Kirschner wire through the
calcaneum (Fig. 3). External fixation with a De Bastiani device was applied on the
femur and tibia (Fig. 4), thus allowing gradual and further extension for the
following 25 days, until complete extension (Fig. 5). The external fixation was
then removed (Fig. 6). The patient started physiotherapy 45 days after surgery.
2. Goodwin N., 7 yr. male
Whole hand involved in scarring process due to burn suffered some four years before.
Severe flexion of hand on forearm (85') with subtotal fusion of palm with anterior aspect
of wrist. Hyperextension of 2nd, 3rd, 4th and 5th fingers at metacarpophalangeal joints.
Hyperflexion of interphalangeal joints.
The wrist scar was excised in general anaesthesia. During this manoeuvre neurolysis of the
median nerve was performed. Particular attention was paid to the nerve, which did not seem
to suffer as a result of the rapid extension. Capsulotomy of the wrist joint and
tendolysis of all the flexor tendons were carried out. The entire ulnar group of muscles
was detached from the epitrochlear and diaphyseal insertions in the ultia, thus allowing
normal extension of the palm and fingers.
On termination of the operation extension was not complete - flexion was still about 25'.
A De Bastiani external fixation was applied, which allowed gradual and progressive
extension in the following weeks.
The external fixation was removed after 30 days, and physiotherapy commenced five weeks
after surgery.
3. Raphael K., 6 yr, male
Burn on dorsum of left foot and distal aspect of leg three years before.
The burn healed spontaneously with no grafting of any sort. The boy presented a 65'
flexion of the foot on the leg. The 5th toe was also hypetflexed. A vertical scar, 2 cm
wide and 15 em long, was present on the posterior aspect of the knee.
The scar in the popliteal area was excised in general anaesthesia and the defect closed
with multiple Z-plasties.
The same procedure, with a simple Z-plasty, was used on the anterior aspect of the ankle,
while the 5th toe was extended with a V-Y procedure and tendolysis of the extensor
tendons.
A splint was applied. The patient was mobilized after 15 days, commencing physiotherapy
and free motion of the extremity.
4. Sueba Z ' 7 yr, female
Burn in lower third of face and upper third of neck two years before. Right arm and
shoulder also burned. Healing achieved without medical treatment, leaving retracting
scars.
The patient presented thick, retracting keloid scars in the mental and submental regions,
and hypertrophic scars in the anterior cushion of the the right axilla and the anterior
aspect of the elbow.
The keloids in the face and neck area were removed in general anaesthesia and the defect
closed with a full-thickness skin graft from the groin. Retractions in the axilla and
elbow were corrected with excision of scars and Z-plasties.
There was no immobilization and the patient was discharged after seven days, with an
invitation to exercise the right arm.
5. Chiesu M., 8 yr, male
Large scar occupying whole dorsum of left foot with median band about 1.5 cm wide
retracting foot in 65' flexion.
A subtotal excision of the scar was performed in general anaesthesia, leaving the skin on
the metatarsal joints and displacing it from the dorsum with a V-Y procedure. The rest of
the defect was covered with a full-thickness skin graft from the groin. The patient was
allowed to walk after two weeks.
6. Edson P, 6 yr, male
Limited but massive scar retraction of 3rd, 4th and 5th finger of right hand, with
complete flexion of metacarpal and interphalangeal joints.
In general anaesthesia the scar was excised, tendolysis of the flexor tendons was
effected, and the defect was closed with a full-thickness skin graft from the groin.
The position of the fingers was maintained with a splint, which was removed after two
weeks allowing free movement of the fingers.
7. Majula G, 48 yr, female
Lady presenting several linear scars on face involving nasolabial folds and cheeks.
In local anaesthesia all the scars were excised at the level of the nasolabial folds and
Z-plasties were performed, positioning the scar line as far as possible on the line of the
fold.Excellent cosmetic results were obtained.
8. Mpande S., 6 yr male
Boy with severe scar retraction in right ankle (45') and knee (120') due to local burn
two years previously.
In general anaesthesia the scar was excised and tendolysis was performed. The defects were
covered with a skin graft from the groin.
The knee retraction was corrected by excision of the scar and Z-plasty.
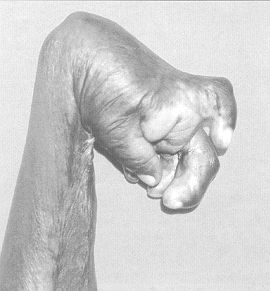
9. Cristabel G 16 yr. female
This girl had suffered a severe burn of the left breast, shoulder, arm, forearm amd
hand five years previously. She presented a distortion of the left breast, which was
smaller than the right breast and entirely covered by scars. There was a moderate scar
retraction in the anterior cushion of the axilla. The anterior aspect of the elbow was
retracted by a linear scar (140'). The left hand was flexed on the forearm (50') with
subtotal adhesion of the palm to the wrist; the 3rd, 4th and 5th fingers wore flexed
tightly on the palm (Fig. 7).
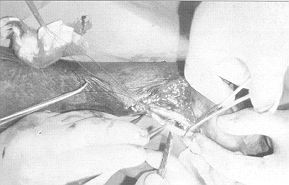
In general anaesthesia, the scar at the wrist was incised, exposing the flexor tendons.
Tendolysis was performed and elongation was obtained by dividing the superficial tendons
distally to the metacarpal joints and the deep tendons proximally to the carpal tunnel,
suturing the distal stumps of the superficial tendons with the proximal stumps of the deep
tendons (Fig. 8). 'lie position was maintained with an external fixation device and
the skin defect at the wrist and palm was grafted with a full-thickness skin graft from
the groins (Fig. 9).
No procedures were performed at this time in the other scar contractures on the hand and
the rest of the upper limb.
The graft took uneventfully and the hand was mobilized after five weeks, when
physiotherapy commenced.
10. Mwanyaly K, 6 yr male
Fifth finger completely flexed because of a linear scar due to a local burn three
years previously.
In general anaesthesia the scar was excised and a multiple Z-plasty was performed.
Immobilization on a Zimmer splint was removed after seven days, leaving the finger free.
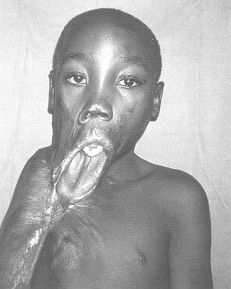
11. Enock G, 10 yr, male
Extremely severe scar retraction due to burn four years previously. Healing achieved
without medical treatment (Fig. 10).
The anterior aspect of the neck was totally involved in the scar contraction, which also
extended in the lateral aspects. The lower lip was displaced by the retraction down to the
central portion of the sternal area (Fig. 11). The jaw was dislocated downwards and
the boy had severe feeding difficulties.
|
Fig. 7 -
Extreme contracture of right hand in girl aged 16 yr following hum suffered in childhood. |
 |
 |
Fig.
8 - Flexor tendons elongated by dividing superficial tendons distally at level of
metacarpal joints and deep tendons proximally to carpal tunnel. |
Fig. 9 -
De Bastiani device applied to maintain and increase extension by daily adjustment of
screw. Raw area on wrist covered with full-thickness skin graft from groins. |
|
The right anterior cushion of the axilla
was severely retracted and the arm flexed on the trunk with no abduction. During the
surgical operation tracheal intubation proved impossible. Intubation via the nose was
repeatedly but unsuccessfully attempted as the trachea was grossly displaced towards the
right side of the neck. The only possible anaesthesia was neuroleptoanalgesia and heavy
sedation.
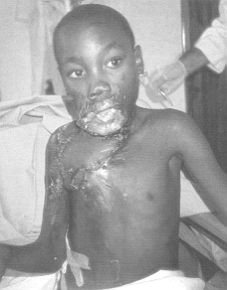
The neck scar was resected, exposing the various elements of the neck. The large defect
was covered by means of a myocutaneous flap of latissimus dorsi, with an island of skin
measuring 25 x 12 em which subcutaneously reached the lower portion of the neck and the
upper part of the thorax defect. The submental and upper parts of the neck defect were
covered with a split skin graft from the right thigh (Fig. 12).
The repositioned lower lip developed considerable oedema which took about a month to
resolve. The boy was able to take any kind of food a few days after surgery. A partial
portion of free skin graft did not take and the patient had a second operation three weeks
later. This time healing was uneventful (Fig. 13).
Discussion
Peacock and Cohen have written:
"wound healing abnormalities are among the greatest causes of human disability,
deformity and even death.
Most of the above cases involved unusual post-burn scar contractures. It is well known
that the process of wound healing, with the production of a normal scar, is the result of
various biological processes which, in order to produce the best possible scar, must
fulfil a number of requirements, without which it is difficult to obtain normal
epithelialization, collagen metabolism, and contraction with a soft but stable scar.
Peacock and Cohen' studied this process extensively. They found that post-trauma
nutritional deprivation and certain types of immunosuppression impair the quality of scar
production. In particular, the role of vitamin A in determining normal contraction was
stressed by Herlich grafts and Hunt' and by Herlich, Tarver and Hunt.' Ascorbic acid
deficiencies and hypoxia also appear to play a role in the production of normal collagen
molecules, as demonstrated by Stein and Keiser' and Cohen and Keiser'.
 |
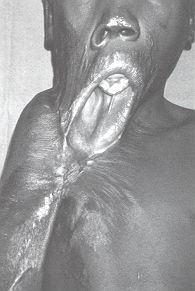 |
| Fig. 10
- Result of spontaneous healing of burn injury suffered four years previously by boy aged
10 yr involving neck, right shoulder and right arm. |
Fig. 11 - Displacement
of lower lip down to thorax and of mandible showing malocclusion of about 2 cm. Right
shoulder also contracted medially and abduction prevented by sear. |
 |
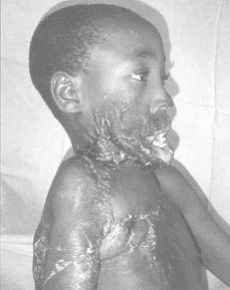 |
| Fig. 12 -
Skin defect following resection of scar on neck and subelavicutar region closed by
latissimus dorsi flap with island of skin measuring 25 x 12 em and with split skin |
Fig. 13 -
After two weeks lower lip still very oedematous. Neck mobile. Right shoulder hypotrophic.
Patient initiated physiotherapy 45 days after surgery after return of Interplast Team to
Italy. |
|
Frank, Brahme and Van der Berg' studied the influence of
splinting and pressure on the regulation of scar contraction.
These and other factors may have interfered with the process of normal scar production in
the patients described in this series. The fact that nutritional deprivation,
hypovitaminosis, anaemia and therefore hypoxia are almost endemic among rural populations
in central Africa most probably accounts for the unusual severity of the contractures.
RESUME. U Auteur présente
les résultats de 11 cas de séquelles de brûlures, principalement dans des enfants,
traitées par une équipe italienne dans l'Hôpital Zambien-Italien à Lusaka (Afrique
centrale). Du point de vue technique les procédures chirurgicales ne présentent pas de
problèmes particuliers, mais dans le contexte social de l'Afrique centrale elles
améliorent la qualité de vie de ces enfants malheureux et bien souvent constituent la
condition sine qua non pour leur survie. En Zambie, comme toute l'Afrique centrale, les
brûlures ne sont pas traitées en manière particulière. Les rares patients qui
survivent sont atteints de contractures des cicatrices extrêmement sévères, avec des
conséquences tragiques. L'Auteur décrit les cas traités et les résultats obtenus.
BIBLIOGRAPHY
- McCarthy J.: "Plastic surgery", 4: 2437.
W.B. Saunders Co.,Philadelphia, 1990.
- Peacock E.E., Cohen J.K.: Wound healing. In:
McCarthy J., "Plastic surgery", 1: 161. W.B. Saunders Co., Philadelphia, 1990.
- Herlich H.P., Hunt T.K.: The effects of cortisone
and anabolic steroids on the tensile strength of healing wounds. Ann. Surg., 170: 203,
1969.
- Herlich H.P., Tarver H., Hunt T.K.: Effects of
vitamin A and glucocorticoids upon inflammation and collagen synthesis. Ann. Surg.,
177:222,1973.
- Stein H.D., Keiser H.R.: Collagen metabolism in
granulating wounds. J. Surg. Res., 11: 277, 1971.
- Cohen J.K., Keiser H.R.: Disruption of healed scars
in scurvy. The result of a disequilibrium in collagen metabolism. Plast. Reconstr. Surg.,
57: 213, 1976.
Frank D.H., Brahme J., Van der
Berg J.S.: Decrease in rate of wound contraction with the temporary skin substitute
Biobrane. Ann. Plast. Surg., 12: 519, 1984.
Acknowledgement
The author wishes to thank Prof. P. Santoni-Rugiu, Senior Surgeon of the Interplast
Team in Zambia, for giving him responsibility for the treatment of the patients in the
series described in this article and for his suggestions and constructive criticisms as
the article was conceived and written.
| This paper was received on 11 March
1996. Address correspondence to: Dr
Daniele Gandini, U.0. Chirurgia Plastica, Ospedale di Cisanello, Via Paradisa 2, 56124
Pisa, Italy (Tel.: 050.596966-596879-596965). |
|