| Annals of Burns and Fire Disasters - vol. IX
- n. 3 - September 1996
USE OF CULTURED HOMOLOGOUS KERATINOCYTES IN THE LOCAL TREATMENT OF LVELUS
SYNDROME
Napoli B.,
D'Arpa N., Masellis M., D'Amelio L., Genovese M.
Divisione di Chirurgia Plastica e
Terapia delle Ustioni, Ospedale Civico, Palermo, Italy
SUMMARY. The
authors describe two cases of toxic epidermal necrolysis (Lyell's syndrome). The first
case did not have a clear pharmacological aetiology, occurring in a patient with a
lymphoproliferative condition (non-Hodgkin's lymphoma). The second patient had taken a
number of drugs and the aetiology was probably attributable to anticonvulsants
(phenobarbital, phenytoin and carbarnazepinc). The cases did not present any complications
and were treated with vitamins, gastroprotective and rehydrating therapy, appropriate
nutritional support, without the use of steroids, and with local application of
cryopreserved cultured homologous keratinocytes which promoted extremely rapid
re-epithelialization of the lesions (48 h). The specific literature regarding both Lyell's
syndrome and the problerns involved in the cultivation of human epithelium are reviewed
and the Authors find confirmation of the biological foundations and the validity of the
local treatment which they applied.
Introduction
Lyell's syndrome resembles a partial-thickness burn because of the presence of erythema
and the formation of bullae, the surface of which consists of the epidermis, with
subsequent detachment exposing the dermal layer of the cutis.
The modifications of the skin covering that
occur in Lyell's syndrome require general and local treatment analogous to that required
in burns. For this reason toxic epidermal necrolysis (as Lyell's syndrome is also known)
is a pathology that is often treated in Burn Centres.
The purposes of the local treatment of Lyell's syndrome are:
- to reduce the intensely painful burning
feeling
- to prevent heat and fluid loss to prevent
bacterial contamination and septic processes to prevent the lesions from becoming deeper
- to promote re-epithelialization
The methods of local
treatment described in the literature (air-fluidized bed,2 hyperbaric oxygen therapy,'
antibiotic and antiseptic treatment,'-' skin substitutes` 14) are not always sufficient to
achieve these purposes. Barring complications, re-epithelialization generally occurs
within two weeks (as in partial-thickness burns) and never in less than a week.
Clinical cases and
methods
We describe here two recent cases of Lyell's syndrome in which we successfully used
cultured homologous keratinocytes for topical treatment.
The homotransplant donors were tested and found negative for Toxo IgG and IgM, CNIV IgG
and IgM, HbsAg and HCV, HIV 1+2, and TPHA.
The patients were subjected to the removal of cutis in negative Nikolsky's sign areas for
laboratory culture and conservation of autologous keratinocytes to be used if necessary as
an autologous dressing in the post-acute phase of the disease.
Patient with non-Hodgkin's lymphoma diagnosed
histologically in 1994. In December 1995, following the appearance of large submandibular
swellings, the patient was given radiation therapy (15 sessions) and pharmacological
treatment (dexamethasone 4 mg per day for 45 days). On 24 March 1996, two days after the
last radiation session, the appearance was observed of rubescence and oedema with
subsequent de-epithelialization in the face and neck, progressively involving the trunk
and upper limbs. The patient was admitted to the Dermatology Department and diagnosed as
suffering from Lyell's syndrome. On 31 March 1996 he was transferred to our division.
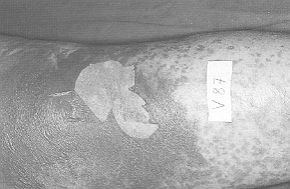
Objective examination
on admission
The face presented lesions in the healing
phase; zones of erythema and de-epithelialization were present in the neck, upper limbs,
trunk, and lower limbs (Fig. 1). Nikolsky's sign was positive. The visible and
explorable mucosae were not affected.
 |
 |
| Fig. 1 |
Fig. 2 |
 |
 |
| Fig. 3 |
Fig. 4 |
|
Diagnosis
The skin biopsy performed on I April 1996 provided histological confirmation of the
clinical diagnosis. The lymphocyte typing was also compatible with the diagnosis (reduced
T lymphocytes with reduced helper- suppressor ratio). Activated lymphocytes present.
Increased NK lymphocytes (CD 16).
Clinical course and treatment
During the course of the disease the patient did not present any blood gas analysis
modifications and chest radiography was normal. Electrolytes remained normal, as also
kidney function (urea and creatininaemia) and liver function (transaminase, bilirubin,
alkali phosphatase).
On admission the patient presented leucopenia
(WBC x 10'/ml 2.53) with neutropenia (62.9%) and thrombocytopenia (P1t x 101/tul 83).
During the course of the disease there was a progressive increase in these values towards
normalization when the patient was discharged (WBC x 101/ml 5.86; neutrophils 72.5%; P1t x
101/mI 123).
Haemocoagulation remained within the normal range.
Swabs from the right hand and neck developed germs which generally contaminate
Lyell's syndrome lesions, i.e. strains of Staphylococcus aureus and epidermidis B-1actamase-producing
and non-producing.
The patient was given vitaminic, antibiotic
and gastroprotective treatment together with heparin prophylaxis and rehydrating therapy.
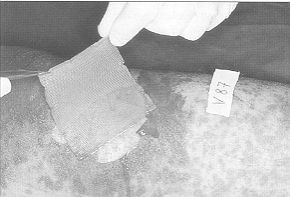
Local treatment
On 1 April 1996 cultured homologous keratinocytes were applied on some
de-epithelialized zones.
The zones presenting only macular erythema
were dressed with dry petrolatum gauze and Desogen tincture. On the same day skin was
removed from a zone with negative Nikolsky's sign and sent to the laboratory for
culturing.
On 3 April the zones dressed with keratinocyte cultures were found to be completely
re-epithelialized.The patient was dismissed on 10 April 1996. Nikolsky's sign was negative
in all body areas.
Case 2 C.M., female, aged 57 yr
The patient, admitted on 31 March 1996 to the Neurology Department and subjected to CT
scan, presented a roundish formation in the right posterior parietal cortical area
surrounded by a clearly visible perilesional oedematous condition. The patient was given anti-oedema therapy
(mannitol, furosemide and dexamethasone) together with gastroprotective therapy (ranitidine) and anticonvulsants
(phenobarbital).
On 1.0 April 1996 the patient was transferred
to the Neurosurgery Department, where the same therapy was continued, with the exception
of steroids, but with double the dosage of phenobarbital (Gardenal 100 mg, two tablets
daily).
Four days later, following the appearance of a diffuse erythematous reaction thought to be
of allergic origin, therapy was continued with steroids (betamethasone, Bentelan, 4 mg, 1
phial twice daily) and antihistamines (dexchlorpheniramine-polaramin AR, one pill twice
daily).
As phenobarbital was considered to be the cause of the reaction, it was suspended and
replaced by phenytoin (Dintoina 100 mg, two tablets daily), with the addition of
carbamazepine (Tegretol 200 rng, two tablets daily).
On 30 April the patient presented a new diffuse erythematous reaction which persisted for
several days, despite the resumption of steroid and antihistaminic treatment and the
interruption of anticonvulsant therapy.
On 11 May the patient was transferred to the Dermatology Department, where the skin rash
became more complicated with the appearance of diffuse bullae and the characteristic
features of Lyell's syndrome.
Four days later (15 May 1996), the patient was transferred to our department.
Objective examination on admission
The patient presented an intense and diffuse macular erythema in the lower limbs,
with a lesser degree of erythema in the abdomen; there was disintegration of the epidermis
in the glutei, arms, and limited areas of the legs (Fig. 5). Nikolsky's sign was
positive in parts affected by macular erythema. The visible and explorable mucosae were
not affected.
 |
 |
| Fig. 5 |
Fig. 6 |
 |
 |
| Fig. 7 |
Fig. 8 |
|
Diagnosis
The clinical diagnosis was confirmed by biopsy on 16 May. The results of lymphocyte typing
were also consistent with the clinical and histological diagnosis (reduced T lymphocytes
with normal helper- suppressor ratio; increased NK lymphocytes [CD 16]).
Clinical course and treatment
This case, like the first, presented an uncomplicated clinical course. Leucocytes and
platelets remained within normal limits. Swabs from the gluteal regions developed strains
of Acinetobacter and Staphylococcus epidermidis not producing B-1actarnase.
The patient was given vitaminic and
gastroprotective treatment, heparin prophylaxis and rehydrating therapy. No antibiotics
were administered and steroid treatment was gradually reduced and in the end suspended.
The patient fed regularly per os.
On 18 May 1996 infusion therapy was suspended and the patient was encouraged to leave her
bed.
Local treatment
On 15 May 1996 (the day of admission to our Department) some de-epithelialized zones were
dressed with cultured homologous keratinocytes.
The zones with macular erythema and initial
formation of small bullae were dressed with dry petrolatum gauze and Desogen tincture. On
16 May skin was removed for culture from a zone with negative Nikolsky's sign. On 17 May
the zones treated with keratinocytes were found to be completely reepithelialized.
The patient was discharged on 27 May 1996.
Nikolsky's sign was negative in all parts of the body.
Discussion
The local treatment of Lyell's syndrome
varies considerably. Apart from hyperbaric oxygen therapy, which is preferred by
reanimators, the choice of treatment ranges from antiseptics and antibiotics to biological
or synthetic skin substitutes.
Antiseptics and antibiotics applied on
extensive areas may cause problems of toxicity due to absorption and some, e.g. silver
sulphadiazine, may even induce Lyell's syndrome; while skin substitutes present problems
of application and require perfect adherence, without which they are ineffective.
The literature relative to Lyell's syndrome does not mention the use of cryopreserved
cultured homologous keratinocytes.
However, bibliographical research into the applications of cultured skin provides evidence
for the biological confirmation of the validity of its use.
De Luca and Cancedda.` found that when burned
areas were covered with homologous keratinocytes the take is only apparent, and that what
in fact occurs is the proliferation and migration of residual keratinocytes in the lesion.
Instead of "take" they use the term "epidermal regeneration", which
better describes the real clinical effect of the application of homologous keratinocytes
(a biological dressing). The stimulus for epithelial regeneration comes from the intense
secretory activity (cytokines, hormones and numerous growth factors) performed by the
homograft sheets; this is the reason for the rapidity of re-epithelialization.
This is the basis found in the literature of the clinical application of cultured
homologous keratinocytes in pathological forms such as ulcers in the lower limbs,
dermo-epidermal graft donor areas, sandwich technique with widemesh net graft, and
superficial and deep dermal burns.`
It was therefore concluded that, like superficial burns, Lyell's syndrome, with its
superficial epithelial necrosis leaving the dermis intact, could benefit from the use of
cultured homologous keratinocytes.
Conclusion
Previously we had
treated cases of Lyell's syndrome in various ways (using antiseptics, antibiotics, dry
petrolatum gauze, and synthetic skin substitutes) with results comparable to those in the
literature.
In the two cases we describe here, both
without complications and not serious, apart from the problem of the advanced age of the
first patient, local treatment with cultured homologous keratinocytes determined
re-epithelialization of the affected areas in only 48 hours and led to complete healing.
Both patients were placed on air-beds (Mediscus).
We would make the following conclusions:
Cultured homologous
keratinocytes should be taken into consideration in the local treatment of Lyell's
syndrome (which we believe should be conservative treatment) in a burns centre with a
laboratory for cell culture.
Skin should be removed
immediately after admission of the patient from areas with negative Nikolsky's sign for
the culturing of autologous keratinocytes. These can then be applied in patients with
complications in the chronicizing phase, in slow-healing areas (e.g. gluteal regions or
other pressure areas) or in cases of recidivation of the disease.
SUMMARY. Les
Auteurs décrivent deux cas de nécrolyse épidermique toxique (syndrome de Lyell). Le
premier cas s'agissait d'un patient sans étiologie pharmacologique évidente qui
présentait une condition lymphoproliférative (lymphome non hodgkinien). L'autre patient
avait pris divers médicaments et la cause probable de la maladie était les
anticonvulsivants (phénobarbital, phénytoďne et carbamazépine). Pour le traitement des
deux cas, non compliqués, les Auteurs ont pratiqué une thérapie vitaminique,
gastroprotective, réhydratante, avec un support nutritionnel approprié, sans l'emploi de
stéroďdes et, localement, l'application d'une couverture de kératinocytes homologues
cultivés et congelés qui a déterminé la réépithélialisation des lésions avec une
rapidité impressionante (48 h). Les Auteurs, aprčs avoir examiné la littérature
spécifique sur le syndrome de Lyell et celle qui s'occupe des problčmes de la culture de
l'épithélium humain, ont trouvé la confirmation des bases biologiques et de la
validité du traitement local qu'ils ont employé.
BIBLIOGRAPHY
- Napoli B., D'Arpa N., Sferrazza Papa G., Masellis
M.: A case of toxic epidermal necrolysis associated with mycosis fungoides and complicated
by consumption coagulopathy. Ann. Medit. Burns Club, 8: 11-16, 1995.
- Revuz J., Laroche L., Touraine R.: Treatment de la
nécrolyse épidermique aiguë (Syndrome de Lyell). Nouv. Presse Méd., 7: 4273-6, 1978.
- Ruocco V., Vimonte D., Luongo C.: Hyperbaric oxygen
treatment of toxic epidermal necrolysis. Cutis, 38: 267-71, 1986.
- Anhalt G., Snelling C.F.T.: Toxic epidermal
necrolysis. Case Report. Plast. Reconstr. Surg., 61: 905-10, 1978.
- Grana G., Barbieri G.C., Malagnino F.C., Pignatti
Morano R., Arisi B., Cimitan A.: Sindrome di Lyell: patologia e approccio
multidisciplinare. Min, Anest., 49: 583-7, 1983.
- Halebian P.H., Madden MR., Finklestein J.L., Corder
V.J., Shires G.T.: Improved burn center survival of patients with toxic epidermal
necrolysis managed without corticosteroids. Ann.
Surg., 204: 503 12, 1986.
Kaufinan T., Schechter H.,
Bar-Joseph G., Hirschowitz B.: Topical treatment of toxic epidermal necrolysis with
lodoplex. J. Burn Care Rehabil., 12: 346-8, 1991,
Pruitt B.A.: Burn treatment
of the unburned. JAMA, 257: 2207-8, 1987.
Ward D.J., Krzeminska E.C.,
Tanner N.S.B.: Treatment of toxic epidermal necrolysis and a review of six cases. Burns,
16: 77-104, 1990.
Artz C.P., Rittembury H.S., Yarbrough D.R.: An
appraisal of allografts and xenografts
as biological dressings for wounds and burns.Ann. Surg., 175: 934-5, 1972.
Heimbach D.M., Engrav L.H., Marvin
J.A., Hamar T.J., Grube B.J.:Toxic epidermal necrolysis. A step forward in treatment.
JAMA,257: 2171-5, 1987.
Kucan J.V.: Use of Biobrane in the
treatment of toxic epidermal necrolysis. J. Burn Rehabil., 16: 324-8, 1995.
Pousa F., Valero J., Vazquez-Barro
A., Trincado S.: Burn unit treatment of three Stevens-Johnson syndrome cases with
cryopreserved allograft. Ann. Medit. Burns Club, 5: 160-3, 1992.
Prasad J.K., Feller I., Thompson
P.D.: Use of amnion for the treatment of Stevens-Johnson syndrome. J. Trauma, 26: 945-6,
1986.
De Luca M., Cancedda R.: Culture of
human epithelium, Burns, 18 (Suppl. 1): S5-S 10, 1992.
RissoD.,MagliacaniG
,StellaM.,MerlinoG.,CalcagniM.,Bergamin F: Cheratinociti alloplastici colturati Conte
copertura temporanea nel grande ustionato. Atti 1 l' Cong. Soc. hal. Ustioni, Bari, 1994.
| This article was
received on 15 June 1996. Address
correspondence to: Dr B. Napoli, Divisione di Chirurgia Plastica e Terapia delle Ustioni,
Ospedale Civico, Via C. Lazzaro, 90127 Palermo, Italy.
Tel.: 39 91 6663635, Fax: 39 91 596404. |
|