| Annals ofBurns and Fire Disasters - vol. IX - n. 4 - December 1996
HAEMATOLOGICAL CHANG IN SEVERELY BURNED PATIENTS
EI-Sonbaty M.A., EI-0tiefy M.A.
Burn Unit, Assiut University Hospital, Assiut,
Egypt
SUMMARY. A
prospective study was undertaken to determine the haematological changes occurring in
severely burned patients. The study included 30 patients (18 females and 12 males), all
with flame burns (range, 30/65% TBSA). Daily estimation of routine haematological
laboratory values was carried out. The individual mean of each of these values in patients
who survived (21 patients) was statistically compared with that of patients who died (9
patients). It was found that laboratory manifestations of anaemia were evidenced six days
postburn and two days earlier in the non-survivors. Leucocytosis was manifested soon after
the bum and was steady in the survivors. The platelet count showed decreased levels in
both groups, with significantly increased levels in the survivors by the end of the first
week.
Introduction
The patient with a major bum has
suffered one of the most severe forms of trauma. The pathological changes produced in the
circulatory and respiratory systems are complex, and failure to understand their progress
and therapeutic management can cause the patient further problems. It is well known that a
severely bumed patient presents the greatest dysregulation of homeostasis of any injury.'
Muir has shown that a general relationship exists between the extent of deep bum and the
amount of red cell destruction.' Baxter observed a shorter life span of red blood cells.'
Enremus reported that 10% of the total red cell mass is injured during the bum process.'
All these changes have been attributed to the presence of some type of detrimental plasma
factor, because when the red cells are injected into a normal person they survive a normal
length of time.'Also, the serum of bum patients contains a substance that inhibits
erythropoiesis.
Peripheral blood phagocytic cells (granulocytes and monocytes) may also be influenced,
with serious consequences for infection resistance, which is known to detenorate in bum
injury.
Thrombocytopenia is almost universal in bacterial infections associated with bacteraernia
and is usually the result of increased platelet consumption. The reduced platelet count
may be an isolated finding or it may be associated with disseminated intravascular
coagulopathy. Thromboeytopenia usually occurs early and can be an early indication of
bacteraernia in bum patients!
Materials and methods
The study included 30 patients (18
females and 12 males), all with flame burns ranging from 30 to 65% TBSA. Their ages varied
between 17 and 47 years (mean, 25 years). In addition to the study groups there was a
control group consisting of ten healthy volunteers of the same age and sex range.
The study group was admitted to the Burn Unit of Assiut University Hospital in the period
January 1992/January 1993. All the patients received intensive care and resuscitation
immediately after admission. Daily determination of blood urea, scrum creatinine, serum
sodium, serum potassium and blood gases was performed during the first week and thereafter
as needed. Daily estimation of erythrocyte count, haemoglobin percentage, haematocrit
value, leucocyte count and platelet count was carried out for the first eight days in both
groups and in the patients who survived until the end of the second week. Other routine
monitoring data were recorded during the period of study. In a trial to identify ominous
parameters during resuscitation of severely burned patients, we made a statistical
comparison between the individual data of the haematological changes in the 21 patients
who survived ("survivors") and those of the nine patients who died
("non-survivors").
Results
Haemoglobin concentrations showed
significantly high levels immediately after the burn, especially in the non-survivors.
This high level decreased gradually to below control level by day 4 post-burn in the
non-survivors and by day 6 post-bum day in the survivors. The same pattern of changes was
noticed regarding haematocrit levels and red blood cell count (Fig. 1).
There was a highly significant leukoeytosis in both groups compared with control.
Leukocytosis in the survivors remained constantly at high levels, while in the
nonsurvivors it showed oscillating levels until death (Fig. 2).
The platelet count, on the contrary, showed a significant decrease in levels below
control, reaching very low levels in the non-survivors, while it increased steadily in the
survivors after day 4 post-bum, reaching levels above control by day 7 post-burn and
thereafter (Fig. 3).
Discussion
The daily estimation of haemoglobin
percentage, haematocrit value and red blood cell count in the severely burned patients in
our study showed that there was progressive anaemia after the initial haemoconcentration
phase and that there was a correlation between the degree of anaemia and burn severity.
These data are consistent with those of Lobel et al.
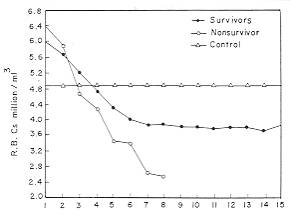 |
Fig. 1 - Mean
values of red blood cell count in survivors, non-survivors and control groups. |
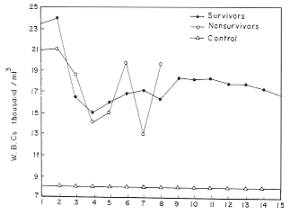 |
Fig. 2 -
Mean values of white blood cell count in survivors, non-survivors and control groups. |
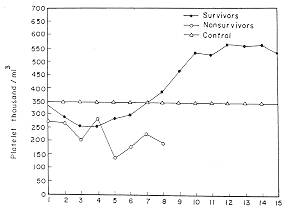 |
Fig. 3 -
Mean values of platelet count in survivors, non-survivors and control groups. |
|
Anaemia in bum patients has been
postulated as being due to the accelerated decomposition of erythrocytes, since a massive
blood transfusion in such patients cannot counter the defect secondary to the effect of
bum-induced factors which cause morphological changes in red blood cells.` The degree of
erythrocyte destruction, measured with radio-labelled chromium, has been shown to be
related to burn severity. The abnormal red cell morphology resembles echinocytes, a form
which is known to result when erythrocyte ATP concentration is depleted," and
follow-up research has found that morphological changes in red blood cells are reversible.
The severely burned patients became severely anaemic by day 4 post-burn, when blood
transfusion had to be initiated in order to replace destroyed red blood cells and to
improve tissue xygenation. Significant leukocytosis was noticed in both survivors and
non-survivors in this study, with constant high levels in survivors.
These findings are consistent with those of most reports. Gruber and Farese reported
peripheral leukocytosis that lasted for 35 days or more in murine granulopoiesis after
inducement of a standardized sublethal third-degree burn.` A similar finding was reported
by D'Alesandro and Gruber in an experimental study on rats, where after a 30% thermal
injury leukocyte quantities were three to five times normal values.` The platelet count
was observed to be significantly increased by day 7 post-burn in the survivors. This in
crease may be considered a good prognostic parameter during the treatment of severely
burned patients. Similar changes in platelet level were reported in D'Alesandro and
Gruber's experimental study. On the contrary, there was a significant and progress ive
decrease in the platelet count in the non-survivors until death ensued. This
thromboeytopenia is usually the result of increased platelet consumption or of decreased
produc tion by bone marrow.
Housinger et al. studied the relationship between plate let count, sepsis and survival in
paediatric bum patients concluding that a decline in the platelet count preceded other
signs of sepsis in all cases and that a platelet count below 0. 1 x 1 O'fl for more than
four days was uniformly associated with death.
In the light of these data, it may be concluded that the monitoring of the platelet count
is of great importance during the resuscitation and care of severely burned patients.
Whenever the platelet count begins to decline, all measures to support the general
condition of the burned patient should be initiated, including the administration of
intravenous fluids and antibiotics, optimal care of the burn wound, debridement or
escharectomy, and blood transfusion.
RESUME. Les Auteurs ont
effectué une étude prospective pour déterminer les modifications hématologiques qui se
produisent chez les grands brûlés. L'étude comprenait 30 patients, dont 18 femelles et
12 mâles, tous atteints de brûlures par flamme (extension, 30 à 65% de la surface
corporelle totale). Les valeurs hématologiques routinières ont été évaluées
journellement en laboratoire. La moyenne individuelle de chacune de ces valeurs chez les
patients qui ont survécu (21 patients) a été comparée statistiquement avec celle des
patients décédés. Les Auteurs ont trouvé que les manifestations en laboratoire de
l'anémie se produisaient six jours après la brûlure (deux jours plus precocement chez
les patients décédés). La leucocytose se manifestait peu de temps après la brûlure et
restait constante chez les patients survécus. Le nombre des plaquettes était réduit
chez tous les patients, mais le niveau chez les patients survécus augmentait en manière
significative avant la fin de la première semaine.
BIBLIOGRAPHY
- Montgomery BJ.: Concept for treatment of the sickest
patients you'll ever see. JAMA, 241: 345-56, 1979.
- Muir I.F.: Red cell destruction in bums, with
particular reference to the shock period. Br. J. Plast. Surg., 14: 273, 1966.
- Baxter C.R.: Problems and complications of burn
shock resuscitation. Surg. Clin. North Am., 58: 1313-22, 1979.
- Enremus K.: Hematologic changes in burns. In:
"Burns: a team approach", 132-48, Artz, Moncrief J., Pruitt B. (Eds). W.B.
Saunders, Philadelphia, 1979.
- Wallner S.E, Vaturin R.M., Seerk C., Robinson W.A.,
Peterson J.M.: The anemia of thermal injury - study of erythropoiesis in vitro. J.
Trauma, 22: 774-80, 1982.
- Miller C.L.: Alteration in macrophage function
following thermal injury. In: "The immune consequences of thermal injury",
49-65, Ninnean J.L. (Ed.). William & Withins, Baltimore, 1981.
- Buffone V., Meakins J.L., Chritou N.V.: Neutrophil
function in surgical patients. Arch. Surg., 119: 39-42, 1984.
- Poskitt T.R., Poskitt P.K.: Thrombocytopenia of
sepsis, the role of circulating IgG containing immune complexes. Arch. Inter., 145: 891-4,
1985.
- Lobel E.C., Morvin J.A., Curred W.P., Baxter C.R.:
Erythrocyte survival following thermal injury. J. Surg. Res., 16: 96-101, 1974.
- Allgower M.: Anaemia. In: "Verbrennungen,
Pathophysiologie, Pathologie, Klinik, Therapie", 88-91, Allgower M., Siefrist J.
(Eds). Springer Verlag, Berlin, 1957.
- Allgower M., Schenenberger, Sparkes B.: Burning the
largest immune organ. Burns, 21: suppl. 1, Sept. 1995.
- Lobel E.C., Baxter C.R., Curred W.P.: The mechanism
of erythrocyte destruction in the early post-bum period. Ann. Surg., 178: 6818,1973.
- Gruber D.F., Farese A.M.: Bone marrow myelopoiesis
in rats after 10%, 20% or 30% thermal injury. J. Burn Care Rehabil., 10: 410-17, 1989.
- D'Alesandro M.M., Gruber D.F.: Quantitative and
functional alterations of peripheral blood neutrophils after 10% and 30% thermal injury.
J. Burn Care Rehabil., 11: 295-300, 1990.
- Housinger T.A., Brinkerhoff C., Warden G.D.: The
relationship between platelet count, sepsis and survival in pediatric burn patients. Arch.
Surg., 128: 65-7, 1993.
This paper was
received on 9 October 1996.
Address correspondence to: Dr M.A.
EI-Sonbaty, Burn Unit, Assiut University Hospital, Assiut, Egypt. |
|