| Annals of Burns and Fire Disasters - vol. IX - n. 4 - December 1996
FACTORS AFFECTING RESULTS IN THERMAL HAND BURNS
Gokalan L,(1) Ozgor F.,(2) Gursu G.,(2) Kecik A.,(2)
(1)Pamukkale University Faculty of Medicine,
Department of Plastic and Reconstructive Surgery, Denizli, Turkey
(2)Hacettepe University Faculty of Medicine, Department of Plastic and Reconstructive
Surgery, Ankara
SUMMARY. One hundred
and seven burned hand deformities reconstructed since 1978 in the clinic of Hacettepe
University Department of Plastic and Reconstructive Surgery (Ankara, Turkey) were analysed
retrospectively and the results evaluated statistically in relation to various factors
(patient's age at time of burn, cause of burn, place of early therapy, degree of
deformity, time of reconstruction, and methods of reconstruction). In the group of mild
hand bum deforn-dties (95), 18 hands were reconstructed with Z-plasties, 65 with
Z-plasties and skin grafts, and 12 with skin grafts. In the group of severe hand burn
deformities (12), five hands were reconstructed with abdominal and groin flaps, four with
forearm flaps, and three with distant flap transfers. The results obtained after ~he
reconstruction of scald burns, domestic accidents, and bums during childhood showed a
better range of motion. Early reconstruction, without any delay pending scar maturation,
was also found to give better results, with greater improvement in range of motion. Hand
deformities as a result of industrial accidents such as chemical burns could not be
satisfactorily reconstructed as these were difficult cases with deep injuries in the
hand's functional units.
Introduction
The hand is used in manipulatory and
exploratory functions, and the upper extremity is thus the most frequently injured part of
the human anatomy. A study of product-related injuries estimated that 36% of these
involved the hand and the upper extremity, and that 39% of burn wounds involved some
portion of the hand and arm.' The proportion of hand involvement was reported as 72% and
85% in two series of burn patients, including electrical burns .2,3 Although some bums are
minor, creating inconvenience rather than a therapeutic challenge, others have a
considerable potential for causing chronic disability and expense variously for patients,
employers and insurance carriers. In a group of 3167 survivors of bum injury, 31% of the
patients required reconstruction for hand bums.' It is thus important that severe burns of
the hands and upper extremities should be managed by physicians with specific knowledge of
burn therapy, reconstruction and rehabilitation in order to maximize the final functional
results .2,5,6 Otherwise, late reconstructions performed because of impaired function are
usually difficult and not always satisfactory in outcome .7,8
This study was conducted in order to
analyse the results of the reconstruction of burned hand deformities and to evaluate
factors affecting the results.
Materials and methods
Seventy-six patients with a total of
107 burned hand deformities reconstructed in the clinic of Hacettepe University Department
of Plastic and Reconstructive Surgery since 1978 were analysed retrospectively. All the
burns were thermal (electrical hand bums were excluded), and all were treated with a view
to reconstruction. The patients received their early care in a number of different
clinics. Following reconstruction they followed a physical rehabilitation programme for
functional recovery. This study analyses retrospectively the history of the patients with
regard to a number of factors, e.g. age at the time of burn, cause of burn, place of early
therapy, degree of deformity, time of reconstruction, and method of reconstruction. The
results were assessed by physical examinations performed in routine controls at yearly
intervals and were grouped on the basis of functional improvement, such as gain in range
of motion. The results were then evaluated statistically in relation to parameters taken
from the patients' history.
Results
Most of the patients had been burned
during childhood before they were Wyears old (77.9% before that age and 22.1% after).
81.6% of the patients had been burned in domestic accidents and 18.4% in industrial
accidents. 13.2% of the patients had been burned with flame, 22.3% had suffered contact
burns due to falling over a stove, 59.2% had been scalded and burned by oil, and 5.3% had
suffered chemical bums. During their early care, 57.8% of the patients had been treated in
an out-patient clinic, 36.9% in a hospital surgery clinic, and 5.3 % in a bums unit.
Out of the 107 hand burn deformities
analysed in this study, 88.8% were classified as mild deformities and 11.2% as severe,
with deep structures affected by the burn injury and a poor active range of motion before
reconstruction.
In 42. 1 % of the cases, the deformed hand
reconstruction was performed within one year of the burn, without waiting for scar
maturation. In the remaining 57.9% of cases, reconstruction was performed later, i.e.
after more than a year.
In the group of mild hand deformities, 95
hands were reconstructed. Eighteen were reconstructed with Z-plasties only (Fig. 1), 65
with Z-plasties plus skin grafts (Fig. 2), and 12 with skin grafts only (Figs.
3,4). In the group of severe deformities, 12 hands were reconstructed with skin flaps (Fig.
5), including five groin and abdominal flaps, four reverse flow forearm flaps, and
three distant free transfers (Table 1).
Method
Number of hands |
|
------------------------------------------------------------------------------------------------------------- |
Mild deformities |
Z-plasties |
18 |
Z-plasties with
skin grafts |
65 |
Resurfacing with
skin grafts |
12 |
| |
Severe deformities |
Groin and
abdominal skin flaps |
5 |
Reverse flow
forearm skin flaps |
4 |
Free tissue
transfers |
3 |
-------------------------------------------------------------------------------------------------------- |
Total |
107 |
|
| Table 1 - Methods used for reconstruction |
|
Results |
Number of hands |
% |
| |
Without any improvement or
limited gain in range of motion |
50 |
46.7 |
Full range of motion |
57 |
53.3 |
| |
Total |
107 |
100,0 |
|
| Table II - Results of reconstruction |
|
The results were
evaluated in two groups: 46.7% of the reconstructions presented no improvement or limited
gain in range of motion, and 53.3% presented satisfactory reconstruction results, with
full range of motion (Table II). results than those in patients burned at a later
age (x 5.59, p <0.02) (Table III). Hand burn deformities in patients burned
before the age of ten years gave more satisfactory reconstruction
 |
 |
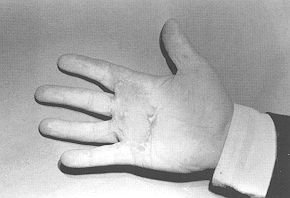
| Fig. la -
Hand burn deformity due to contact burn with flexion contraclure on palmar surface of 3rd,
4th and 5th metocarpophalangeal joints (14-year-old boy). |
Fig. 1b -
After release of contracture by multiple Z-plasties. |
 |
 |
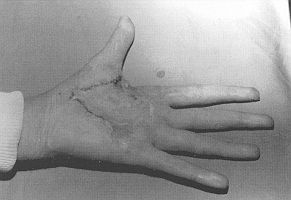
| Fig. 2a
- Hand bum defon-nity due to scalding with flexion contracture on palmar surface of 2nd,
3rd, 4th and 5th fingers (12-year-old girl). |
Fig. 2b - After
reconstruction by contracture release with Z-plasties and full-thickness skin grafts. |
 |
 |
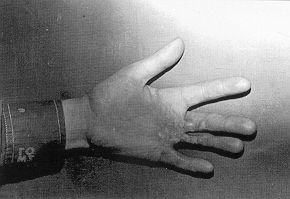
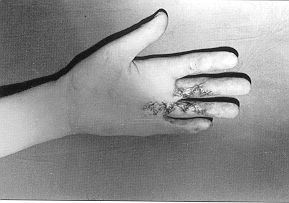
| Fig. 3a -
Hand burn deformity due to contact burn with flexion contracture on palmar surface of 2nd,
3rd, 4th distal metacarpal area (13-yearold boy). |
Fig. 3b - After
reconstruction by resurfacing with full-thickness skin grafts. |
 |
 |
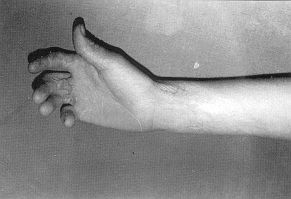
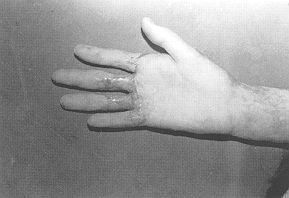
| Fig. 4a -
Hand bum deformity due to scalding with palmar contracture altering thumb motion (21
-year-old woman). |
Fig. 4b - After
reconstruction by contracture release and surfacing with full-thickness skin graft. |
 |
 |
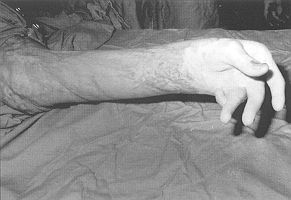
| Fig. 5a -
Severely deformed hand following flame burn with flexion contracture and ulnar deviation
of fingers and stiff joints (54-year-old woman). |
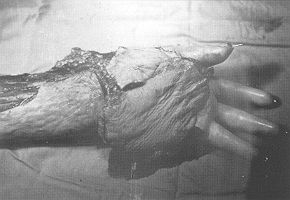
Fig. 5b -
Contracture released without excision, and palmar tissue defect covered by reverse flow
radial forearm flap. still present. |
|
Age
at burn |
Limited
functional gain |
Full range of
motion |
Total |
|
|
|
|
< 10 years |
30 |
47 |
77 |
| > 10 years |
20 |
10 |
30 |
Total |
50 |
57 |
107 |
|
| Table III - Effect of patient age at time of burn on results |
|
Reconstruction results were more satisfactory in
deformities caused by domestic accidents than in deformities caused by industrial
accidents (x = 9.18, p <0.01) (Tqble IV).
Aetiology |
Limited
functional gain |
Full range
of motion |
Total |
| |
|
|
|
Domestic
accidents |
29 |
49 |
78 |
Industrial
accidents |
21 |
8 |
29 |
|
|
|
|
Total |
50 |
57 |
107 |
|
| Table
IV - Effect of aetiology of burn on results |
|
The place of early treatment, i.e. where initial care
was provided, was found to be unimportant as regards the final results of hand burn
reconstruction (x = 0.768, p A.05) (Table V).
Place of early care |
Limited range
of motion |
Full range
of motion |
Total |
|
Out-patient
clinic |
22 |
28 |
50 |
Surgery clinic |
22 |
27 |
49 |
Burns unit |
6 |
2 |
8 |
|
Total |
50 |
57 |
107 |
|
| Table
V - Effect of place of early care on results |
|
The results varied significantly in relation to the
degree of deformity (x = 13.09, p <0.00l): most of the mild deformities resulted
in full range of motion, while severe deformities resulted in limited functional
improvement (Table VI).
Degree
of deformity |
Limited range
of motion |
Full range
of motion |
Total |
| |
Mild |
38 |
57 |
95 |
Severe |
12 |
- |
12 |
| |
Total |
50 |
57 |
107 |
|
| Table
VI - Effect of degree of deformity on results |
|
Burned hand
deformities reconstructed within one year gave better results than those reconstructed
after more than one year (x = 11.20, p <0.001) (Table VII).
Time of reconstruction |
Limited
range
of motion |
Full range
of motion |
Total |
| |
|
|
|
Within
one year |
12 |
33 |
45 |
After
one year |
38 |
24 |
62 |
| |
|
|
|
Total |
50 |
57 |
107 |
|
| Table VII - Effect of time of reconstruction on
results |
|
Discussion
Thermal injuries are characterized by
varying degrees of damage to the skin and underlying structures, depending on the
temperature and type of the heat source, the duration of exposure, and the area affected
by the heat. The aetiological factors can be classified as flash burns, flame burns,
contact burns, and scalds .2~9 In this study most of the hand deformities occurred as a
result of domestic accidents, caused by flame, falling over a stove (especially during
childhood), and scalds.
The large number of domestic burns involving children emphasizes the importance of
education regarding the concept of prevention, with especial attention to young people,
and the need to improve burn safety products.
Improper care during the acute phase may lead to secondary deformities that could
otherwise have been prevented. During hand burn treatment, if attention is paid to basic
principles, if care is taken to eliminate oedema by mobilization, if infection is
prevented by topical antibacterials, and if the burn wound is covered early by tissue
replacement (when necessary), then the hand will most likely regain good functionality.
2,5,6,9 Unfortunately, not all patients present to a plastic surgeon immediately after
they have suffered a hand burn.' Many are seen in the acute phase by health operators who
do not give high priority to hand function, while some patients have such severe total
body surface area burns that appropriate care for the hands comes too late to prevent
deformity.' During the early acute phase the patients in this study were treated in a
number of different clinics where the health personnel were not specialized in hand burn
care and therefore had no specific knowledge of hand wound healing or the prevention of
post~bum hand deformities. A clear understanding of wound healing and scar contracture and
a good knowledge of the management of hand burns are essential if any sense is to be made
of the myriad of deformities that may be encountered. In our group of reconstructions
there was no relation between the final results and the health services where the patients
had originally been treated as these did not differ as regards the quality of the health
personnel and their care and management of the hand burns. Even burns unit personnel who
are accustomed to dealing with major burns may pay little attention to hands as they are
more concerned with the patients' systemic problems.
In the vast majority of patients the initial thermal injury is limited to the skin alone;
the underlying tendons and joints are usually spared. Prolonged wound healing, with its
attendant oedema, infection, fibrosis and immobilization, can lead to secondary joint
contractures, rupture of extensor tendon mechanisms, and adhesion of gliding tissues. In
general, however, it is remarkable how often the deep structures are spared, particularly
in children. This may explain why better reconstruction results have been obtained in
post-burn deformities in children, despite certain difficulties presented by children's
generally low attendance at physical therapy programmes and by some resistant deformities,
such as the inhibition of bone growth following epiphyseal plate destruction. The better
results of childhood hand burn deformities may also be related to the fact that such
lesions are usually superficial contact burns and scalds, while in older patients the
lesions are often due to deep flame bums or chemical burns sustained in industrial
accidents.
Post-burn hand deformities can be difficult to analyse as acute injuries vary widely,
early treatment is often less than optimal, and there are frequently multiple problems in
each hand. For the sake of discussion and treatment, it is helpful to divide these
deformities into categories of different degree, all of which may be present in a single
hand. Soft tissue deformities, including deformities of the dorsal and volar skin surface,
joint deformities with or without tendon injury, and amputations can be regarded as mild
deformities. Bad injuries leading to complex deformities including all the above, plus
tendon and even bone defects, can be classified as severe: it is difficult to reconstruct
these deformities, which usually give rise to poor functional improvement. Fortunately,
however, these are rare. In our study only 11.2% of the deformities concerned
severely burned hands; they were very poor in their active range of motion before
reconstruction, and even after reconstruction functional improvement was unsatisfactory.
For these reasons we can affirm that better results were achieved after mild post-burn
hand deformities.
Once the complex injury has been dissected into its components, the physician, patient,
vocational rehabilitation worker and employer can meet as a team and decide what
procedures have priority in returning the injured patient to work. The hand surgeon must
be aware of the other parts of the body with burn deformities that may necessitate
surgery. A time-related plan with specific recovery goals is imperative because it has
been shown that if patients do not return to work within a certain length of time
following injury, their chances of employment are reduced." The logical approach is
thus to make a careful record of all the anatomical abnormalities secondary to the burn
injury. If patients are to return rapidly to their work and normal daily life, the hand
has to be reconstructed as soon as possible. In this study, reconstruction times were not
planned on the basis of sear maturation, and we found that the results of reconstruction
performed after a year, when scars were mature, were not better than reconstructions
performed earlier. The reacquisition of functional capacity as soon as possible is an
important factor in the prevention of joint stiffness and tendon adhesion, and thus in the
achievement of better results.
In the reconstruction of the burned hand, each case must be carefully evaluated in the
context of total patient care: only then can the best individual procedure or treatment
plan be chosen. As the fundamental problem is the loss of surface covering, it is usually
necessary to add skin by skin grafts or flaps when dealing with the reconstruction of
post-burn deformities. Z-plasties and other local flap procedures often do not provide
enough tissue and they present a higher complication rate when performed in the context of
scars and increased tension. Further stable tissue coverage must therefore be added. The
entire scar should be removed, and any residual contracture released. Usually replacement
or resurfacing with skin grafts is satisfactory. Flap coverage may occasionally be
necessary if further reconstruction for deep structures such as tendons or joints is
planned. Deep structures injured at the time of burning, or ignored during the phase of
acute management, may give rise to chronic problems which are a challenge in
reconstruction, such as joint subluxations or deviations resulting from imbalance in
ligaments and muscular forces. In severe deep burns, tissue transfer, even with free
tissue, is not sufficient to improve hand function as long as tendon and joint problems
still exist. This limiting effect on functional recovery explains why the reconstruction
of severely burned hands may be unsuccessful.
Conclusion
Hand burn deformities are usually
difficult cases for reconstruction. The results depend above all on the type of burn and
the level of the injury. If deep structures such as tendons, ligaments and joints have
been affected directly by the bum, or if secondary infection and joint stiffness develop
as a result of improper initial therapy, the reacquisition of a full range.of motion after
reconstruction is not always possible. It can therefore be concluded that the correct
initial treatment of hand bums is a matter of great importance for the avoidance of
secondary deformities, as it guarantees hand function more surely than reconstruction.
RESUME. Les Auteurs, après
avoir réalisé une analyse rétrospective des 107 difformités de la main brûlée
reconstruites depuis 1978 dans la clinique du Service Universitaire de Chirurgie Plastique
et Reconstructive Hacettepe (Ankara, Turquie), ont effectué une analyse statistique des
résultats par rapport à divers facteurs (l'âge du patient au moment de la brûlure,
cause de la brûlure, lieu de première thérapie, degré de difformitè, temps de
reconstruction, et méthodes de reconstruction). Dans le groupe de difformités légères
de la main brûlée (95 cas), 18 mains ont été reconstruites avec des plasties en Z, 65
avec des plasties en Z et des greffes cutanées, et 12 avec des greffes cutanées seules.
Dans le groupe de difformités sévères de la main brûlée (12 cas), cinq mains ont
été reconstruites avec des lambeaux abdominaux et inguinaux, quatre avec des lambeaux
d'avant-bras, et trois avec des lambeaux à distance. Les résultats obtenus après la
reconstruction des brûlures par ébouillantement, les accidents domestiques et les
brûlures des enfants ont indiqué une capacité meilleure des mouvements. Aussi la
reconstruction précoce, sans attendre la maturation des cicatrices, a montré des
résultats meilleurs, avec une amélioration supérieure des mouvements. Les difformités
de la main dues aux accidents industriels, comme les brûlures chimiques, présentaient de
gros problèmes pour la reconstruction parce qu'il s'agissait de cas difficiles, avec des
lésions profondes des éléments fonctionnels de la main.
BIBLIOGRAPHY
- Salisbury R.E., Dingeldein G.P.: The burned hand and
upper extremity. In: "Operative hand surgery", 2007-31, Green D.P. (Ed.). W.B.
Saunders, New York, 1993.
- Groenevet E, Kreis W.: Burns of the hand. Netherl.
J. Surg., 37:167-73, 1985.
- Melhorn J.M., Horner R.L.: Burns of the upper
extremity in children; long-term evaluation of function following treatment. J. Pediatr.
Orthop., 7: 563-7, 1987.
- Prasad J.K., Bowden M.I., Thompson P.D.: A review of
the reconstructive surgery needs of 3167 survivors of burn injury. Burns, 17: 302-5, 1991.
- Frist W., Ackroyd F., Burke J., Bondoc C.: Long-term
functional results of selective treatment of hand bums. Am. J. Surg., 14: 51621,1985.
- Kealey G.P., Jensen T.K.: Aggressive approach to
physical therapy management of the burned hand. A clinical report. Phys. Ther., 68: 683-5,
1988.
- Graham T.J., Stern P.J., True M.S.: Classification
and treatment of postburn metacarpophalangeal joint extension contractures in children. J.
Hand Surg., 15A: 450-6, 1990.
- Groenevelt F., Schoorl R.: Reconstructive surgery of
the postburn boutonniere deformity. J. Hand Surg., I I B: 23-30, 1986.
- Donelan M.B.: Reconstruction of the burned hand and
upper extremity. In: "Plastic Surgery", 5452-81, McCarthy (Ed.). W.B. Saunders,
Philadelphia, 1990.
- Alperovitch R., Haddad R.: Les btulures de la main
chez 1'enfant. Etude retrospective de 137 dossiers de 1973 it 1982 repr6sentant 177 mains.
Chir. Pediatr., 25: 43-7, 1984.
- Batchelor J.S., Vanjari S., Budny R, Roberts A.H.N.:
Domestic ironbums in children: a cause for concern? Bums, 20: 74-5, 1994
- Helm P.A., Steven C.W., Sarah A.P.: Return to work
following hand burns. Arch. Phys. Med. Rehabil., 67: 297-8, 1986.
- Bowden M.L., Thompson P.D., Prasad J.K.: Factors
influencing return to employment after a bum injury. Arch. Phys. Med. Rehabil.,
70:772,1989.
- Robson M.C., Smith D.J., Vanderzee A.J., Roberts L.:
Making the burn hand functional. Clin. Plast. Surg., 19: 663-71, 1992.
Robson M.C., Smith D.J.: Burned
hand. In: "Plastic Surgery: Principles and Practice", 781-802, Jurkiewicz M.J.,
Krizek T.J., Mathes S.J., Ariyan S. (Eds). CX Mosby, St Louis, 1990.
This paper was
received on 20 May 1996.
Address correspondence to: Prof.
Inci G6kalan, Pamukkale University Medical Faculty, Hastanesi, Doktorlar cad., 20100
Denizli, Turkey (Fax: 00 90 258 263 08 27). |
|