| Annals ofBurns and Fire Disasters - vol. IX - n. 4 - December 1996
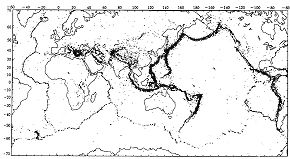
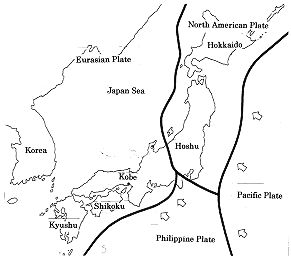
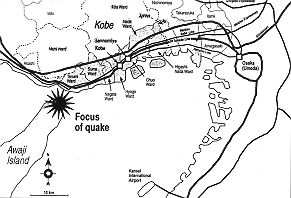
PROBLEMS OF EMERGENCY MEDICAL CARE AT THE TIME OF THE GREAT HANSHIN-AWAJI EARTHQUAKE Ukai T. Osaka City General Hospital, Osaka, Japan SUMMARY. The distinguishing characteristic of the Great Hanshin-Awaji earthquake which hit Kobe and its vicinity in the early morning of 17 January 1995 was that the tremor directly affected a highly urbanized city and revealed the fragility of human life in a sophisticated modem metropolis. The scope of the damage included damage to medical facilities. The difficulties encountered in the early relief activities are also reported. Introduction Some parts of the world are particularly prone to earthquakes (Fig. 1). As Japan is located on the Pacific seismic and volcanic rim, it has been hit by a number of earthquakes in the past. Japan lies over four tectonic plates: the North American Plate, the Pacific Plate, the Philippine Sea Plate, and the Eurasian Plate (Fig. 2). The Pacific Plate and the:Philippine Sea Plate are moving slowly beneath the other two, and when the distortion between the plates reaches a certain extent parts of the plates break and release accumulated energy, causing earthquakes. This is the tectonic type of earthquake. Most earthquakes occurring in and around Japan are of this type. Some violent tremors were not however tectonic but of the direct hit type, caused by the movement of active faults not along the border of tectonic plates. The Great Hanshin-Awaji Earthquake which hit Kobe and its vicinity with a magnitude of 7.2 on the Richter scale at 5.46 am on 17 January 1995 was a direct hit earthquake. As this area had not been struck by a big earthquake for about 400 years, the local residents were not prepared for such a tremor, in spite of warnings given~by seismologists several years ago. Medical facility managers and hospital administrators were also unprepared. The damage The epicentre of the earthquake was
about 14 km under the northern tip of Awaji Island, which is only about 20 km from
downtown Kobe.' The earthquake that hit Kobe, one of the world's largest port cities, was
of the shallow and direct hit type. The most severely damaged area was the central and
eastern part of Kobe (Ashiya and Nishinomiya) (Fig. 3).This area is highly
developed and with Osaka forms the second largest metropolitan area in Japan. It is a very
popular residential area with a mild climate, beautiful scenery, and good transport
connections.
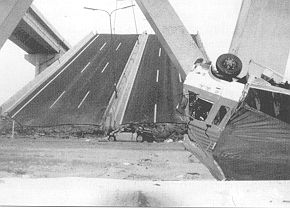
The violent tremor lasted 20 seconds or
less, but 101,233 houses were completely destroyed and about the same number
semi-destroyed. The old wooden houses with heavy tiled roofs collapsed, blocking the
streets and obstructing rescue and relief activities (Fig. 4). Reinforced concrete
buildings built according to the old construction code were also damaged (Fig. 5), but
those built according to the revised construction standards of 1981 did not suffer serious
damage.
The tap water supply was cut off in 1,260,000 households, the city gas service in 845,000 households, and electricity in one million households. As for the telephone service, 285,000 lines were disrupted; the number of calls to the affected area increased to 50 times the usual level, causingan overload on the switchboard circuit. Telephone calls to the disaster area were thus almost impossible on the first, the second and even the third day following the disaster. The final death toll was 6,308, including secondary deaths in some way related to the tremor. About 35,000 persons were injured. 316,678 inhabitants were evacuated to 1,153 temporary shelters. According to the report of Dr A. Nishimura of Kobe University, Department of Forensic Medicine, the most frequent cause of death was traumatic asphyxia (53.9%), followed by crush injury in the chest or the whole body (12.5%). The third most frequent cause of death was burns and CO poisoning (12.2%).' In some cases, when the bodies were charred, it was impossible to judge whether the victims had died before the fire or had been burned to death. Problems of emergency care Overwhelming casualties As so many houses were destroyed and
persons trapped all at the same time, with numerous fires breaking out, the emergency
calls to the local fire departments overwhelmed their capacity. In spite of the maximum
efforts of rescue personnel, paramedics and ambulance crews, it was impossible to respond
to every call. In some places people had to dig out buried family members or friends
almost with their bare hands. On-site triage of the casualties by professional rescue and
ambulance workers was almost impossible. Damage to medicalfacilities Damage to medical facilities was a
serious problem. Out of the 180 hospitals in the disaster area, four were completely
destroyed and 110 suffered serious structural damage. The 1,809 clinics in the area were
similarly affected. Most of the sophisticated medical equipment, such as magnetic
resonance imaging apparatuses, computed tomography, X-ray angiography apparatuses and
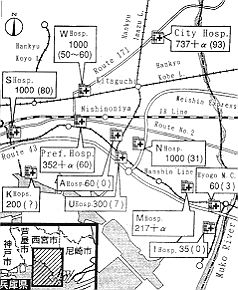
chemical autoanalysers, was damaged and unserviceable. Breakdown of telecommunication systems As said, telephone lines were damaged or overloaded, with the result that this form of communication between hospitals was difficult in the first two or three days. The hospitals were not equipped with any form of radio communication system. On the first day, most of the medical personnel in the disaster area did not know that the hospitals in Osaka, only 20-25 km from the disaster area, had suffered no damage. TV news programmes showed scenes of fires and destroyed highways, but did not give any information about the chaos in the hospitals or about undamaged hospitals. Traffic congestion The widespread destruction of streets, highways, bridges and railways caused severe traffic problems. Within an hour of the tremor every practicable road in the disaster area was full of cars with people leaving the area or on their way to visit family members to ascertain their safety -some even on their way to work. It was not uncommon to take several hours to drive 10 km. These conditions delayed the mobilization of relief teams from neighbouring areas and complicated the transportation of casualties. Disproportionate number of patients in relation to medical facilities available Although the hospitals in the central disaster area were extremely crowded, very few casualties were taken to hospitals outside the disaster area which had suffered no damage. For example, small to medium-sized private hospitals in Nishinomiya (south, west and north), which have 150 to 190 beds, were overwhelmed with more than 1,000 patients each on the first day. On the contrary, only about 60 patients presented at the Hyogo Medical College Hospital, which has about 1,000 beds and is located not many kilometres from the severely damaged area (Fig. 8). With the interruption of telecommunication systems and the serious traffic jams, a journey even of only a few kilometres was regarded as an infinite distance by the general public and ambulance crews. Delay in transportation ofpatients between hospitals Because of the traffic congestion and the lack of appropriate information exchange between medical facilities, the transport of severely injured patients from damaged hospitals to unaffected hospitals was somewhat delayed. When the severity of the damage in Kobe was reported on TV news programmes, most of the tertiary emergency centres in Osaka prepared beds to receive large numbers of casualties. But in the first twelve hours only three patients were transferred to these emergency centres. Crush syndrome and other pathologies The characteristic pathologies of the patients injured or killed in the earthquake were:
In the first two or three days some crush
syndrome patients died or developed shock, serious arrhythmia, acute renal failure, and
compartment syndrome. When however these patients were brought to hospital soon after
extrication their vital signs tended to be stable at first, and in many cases no apparent
external traumas were visible. But for the use of the Foley bladder catheter and the
testing of serum potassium and creatinine kinase levels, the clinical diagnosis of crush
syndrome would have been difficult for physicians without specific trauma centre training. Health problems of the displaced persons At the peak point of the disaster,
more than 310,000 persons were evacuated from their homes to temporary accommodation
centres, such as schools, gymnasiums and other public buildings. There was no electricity,
water or gas supply for several days and even weeks in these temporary shelters. Minimum
supplies of food, clothes and blankets were soon provided, but sanitary conditions in such
circumstances were far from perfect. The earthquake occurred in the coldest season of the
year, and many persons caught cold while living in the shelters. In the early stages most
clinics were closed and could not provide primary health care services for evacuees. Discussion The Great Flanshin-Awaji Earthquake
was certainly unprecedented for Japanese people, not in its scale but because it affected
the country's most highly developed modern city and revealed the vulnerability of human
lives in a metropolis. The disruption for weeks and months of vital public services such
as water supply, electricity, city gas, sewerage, garbage collection, telephone services
and public transport made people's lives in the urban area intolerable. Disaster response
plans defined at the level of national and local government did not at first function
properly because the core organization (city government and prefecture government) failed
to respond in the early phase. Lack of information and the breakdown of telecommunication
systems led to disorganization of the disaster response. Medical services were also
disrupted, The social groups most severely affected were the elderly and the handicapped -
in collective areas of temporary accommodation, senior citizens over the age of 65 yr
accounted for more than half the population. This social group therefore requires careful
attention. RESUME. Uaspect caractéristique du grand tremblement de terre de Hanshin-Awaji qui a atteint Kobe et ses alentours tôt le matin du 17 janvier 1995 a été que le séisme a touché directement une cité fortement urbanisée et a révélé la fragilité de la vie humaine dans une sophistiquée métropole moderne. Aussi les structures médicales ont subi des dégâts écrasants. UAuteur décrit en outre les difficultés des premiers secours. Acknowledgement. The author would like to thank Prof. S.W.A. Gunn and Prof. M. Masellis for inviting him to the 9th Meeting of the Mediterranean Club for Bums and Fire Disasters and allowing him to present a report on the Hanshin-Awaji earthquake. BIBLIOGRAPHY
|