 |
Egypt.
J. Plast. Reconstr. Surg., Vol. 22, No. 2, 1998: 229 - 238 |
Reconstruction
of Post-Burn Axillary Scar Contractures A Surgical Approach
SAMY A. M. SHEHAB EL-DIN, M.D. and
OSAMA M. SHOUMAN, F.R.C.S.
The Plastic, Reconstructive and Burn Unit, Faculty of Medicine, Mansoura
University.
ABSTRACT
Our study included
35 patients with postburn axillary scar contractures. The patients were admitted to the
Plastic, Reconstructive and Burn Unit, Mansoura University Hospitals, from October, 1994
through October 1997. The axillary contractures were classified into 4 types: Type (I):
Linear webs at either the anterior or posterior axillary fold with minimal adjacent
scarring and no involvement of the hair-bearing area. Type (II): Scar contractures
involving either anterior or posterior axillary fold, with adjacent skin scarring but
sparing the hairbearing area. Type (III): Linear webs at both anterior and posterior folds
without involvement of the adjacent skin or hair-bearing area. Type (IV): Involvement of
the hair bearing area. The surgical procedures applied were five flap Y-V advancement and
Z-plasty, for type 1 axillary contractures, inner arm pedicled fasciocutaneous flap and
lateral thoracic pedieled fasciocutaneous flap for type II axillary contractures and
parascapular island fasciocutaneous flap for type III and IV axillary contractures. The
results were satisfactory and the complications were minimal.
INTRODUCTION
Deep partial- and full-thickness burns of the axillary region can result
in scar contractures which limit motion at the shoulder joint, especially abduction and
extension. In order to minimize or prevent axillary contractures, the initial management
of bums in this region should include proper positioning of the shoulder joint in an
abduction splint and aggressive physiotherapy [1]. Early surgical excision and skin
grafting of deep and full-thickness burns will further minimize the development of
contractures [2]. Active and passive excercises and the application of pressure garments
after wound healing and/or graft take are essential in management of these injuries [3,4].
In spite of all these preventive measures, some patients nevertheless develop axillary
contractures. Once scar contracture is established, immediate surgical correction must be
performed to prevent further involvement of the underlying structures [5]. The goal of
surgical correction of axillary scar contractures is to provide maximum correction with
minimum or no local anatomic distortion. Once surgical correction is indicated, the choice
of procedure must be individualized in order to achieve this goal. In this article, we
present our surgical approach in the reconstruction of postburn axillary scar
contractures.
Local
anatomic conditions:
The main problem of axillary contractures is the inelasticity of either or both of the
axillary folds which prevents the full extension and/or abduction of the shoulder joint.
In addition to the scarring of the fold (s), there are two local anatomic conditions that
must be taken into consideration when surgical correction is contemplated. They are: (1)
the amount of scarring of the adjacent skin and (2) the involvement of the hair-bearing
area of the axilla. It is unusual for the hair-bearing area to be involved in thermal
injury due to its anatomic location and because in most instances, the upper extremities
are maintained in adduction, protecting the axillary hair-bearing area [5].
Classification:
Hanumadass et al. [5] have classified the axillary contractures into four types:
- Type I: Is characterized by a linear web at the anterior or
posterior axillary fold with minimal adjacent scarring and no involvement of the
hair-bearing area.
Type II: Is characterized
by scar contractures involving either anterior or posterior axillary folds with adjacent
skin scarring, but sparing the hair-bearing area.
Type III: Is characterized
by linear webs at both anterior and posterior folds without involvement of the adjacent
skin or hair-bearing area.
Type IV: Is characterized by
involvement of the hair-bearing area.
PATIENTS AND
METHODS
Patients
population:
This study included 35 patients (14 males & 21 females) with postbum axillary scar
contractures as outlined in table (1). These patients were admitted to the Plastic,
Reconstructive and Bum Unit, Mansoura University Hospitals, Egypt, from October 1994
through October 1997. The mean age was 15.6 years with a range of 4.5-31 years. The mean %
TBSA bum was 23.3% with a range of 10-40% 'and the mean % of full-thickness burn was 12.5%
with a range of 5-25%. The mean time from initial burn to release being 3.3 years (range
0.5-13 years). All releases were performed electively with the most common etiologies of
burn injury were flame 25 or scald 10 (Table 1).
Surgical Procedures:
The surgical procedures applied were fiveflaps Y-V advancement and Z-plasty, inner arm
pedicled fasciocutaneous flap, lateral thoracic pedicled fasclocutancous flap and
parascapular island fasclocutaneous flap. All patients had photographs taken of the
involved axilla before and after surgery.
The five-flaps procedure
[6]:
The triangular flaps of 2 Z-plastiesand Y-V advancement flap constitute the five-flaps
and their design is shown in Fig. (1). The flap CDE encloses the apex of the axilla and
its tip D lies at the midpoint of the line AB which runs along the ridge of the web. GA
and HB complete the outline of the 2 Z-plasties; the angles 1 & 2 are about 60'. The
incision DF opens into a triangular defect into which CDE is advanced. The part which is
advanced and the only part undermined lies on the undersurface of the web and thus no
change in position of the axillary apex occurs. The length DF is adjusted for the best
fit. Because the ridge of the web is curved, the angles ADF & BDF are slightly larger
than 90� and some trimming of excess may be necessary.
Lateral Thoracic Pedicled
Fasciocutaneous Flap [7]:
The main band of contracture is cut across two-thirds of its width, the incision
continuing one edge of the scar. A kite-shaped defect results. A flap large enough to fill
the defect is raised in the remaining one-third through scar (or skin graft) and deep
fascia. The integument is not disturbed from its attachment to the deep fascia. A length:
breadth ratio of 3:1 is perfectly safe. It is important that the base of the flap is
coterminous with the remaining edge of the scar so that full release of the contracture is
effected. In less severe contractures the secondary defect can usually be closed by
suture. If this results in unacceptable tightness a skin graft may be applied. However,
this should be avoided if possible as the graft may be unsightly because of the deep
secondary defect and the graft's consequent adherence to muscle.
The inner arm pedicled
fasciocutaneous flap [8]:
An incision is made to completely release the tight contracture on the anterior
surface of the axilla, extending onto the deltoid area and the arm is then adducted. A
simple transposition flap, based proximally, is then raised deep to the deep fascia of the
upper arm and avoiding cutaneous nerves wherever possible. This fascia is carefully
separated from the intermuscular septum. In all cases, the dimensions of the flap exceeded
the 2:1 length-breadth ratio. By fishtailing the incision to release the contracture, it
was frequently possible to obtain extra relaxation and in these cases the distal end of
the flap was similarly fishtailed to accommodate the defect. The donor site was closed
primarily. A thin corrugated drain was placed beneath the flap to emerge at the point of
transposition. The secondary defect was dressed, while the flap was left uncovered to
permit inspection. A simple abduction splint was fashioned at the time of operation and
remained until the stitches were removed around the tenth day.
Parascapular island
fasciocutaneous flap [9,10]:
With patient in the lateral decubitus position, the arm abducted at 90 degrees, the
emerging of the pedicle is first determined by accurate location of the omotricipital
space at the lateral edge of the scapula. This space is easily palpable, or one can use
the following measurement procedure. The omotricipital triangle is usually located at
distance DI from the middle part of the spine of the scapula, given by the formula D1 =
(D-I)/2, where D is the distance between the middle part of the spine and the tip of the
scapula.Once the omotricipital space is located, the main axis of the flap is outlined
along the lateral border of the scapula. The upper edge of the flap is outlined at the
same level as the emerging of the pediele. The lower edge can be situated as far as 25 to
30 cm from the upper edge. The width of the flap consistent with closure by direct
approximation is about 15 cm. For such a width, wide undermining of the surrounding skin
and release of tension on the suture line by numerous deep mattress sutures are
necessary.The cutaneous parascapular artery is a terminal branch of the circumflex
scapular artery emerges from the scapular artery out at 4 cm from its origin from the
axillary artery. It divides into one infrascapular branch, which runs horizontally towards
the subscapularis muscle and one descending branch which runs backwards and emerges
posteriorly from the omotrielpital space right at the edge of the lateral border of the
scapula. The descending branch divides into the cutaneous scapular artery, which runs
horizontally over the posterior aspect of the scapula and the cutaneous parascapular
artery, which proceeds to the tip of the scapula that it overreaches.At operation, the
contracture was released by transverse incision of the scar tissue until unrestricted
range of motion was obtained in the shoulder joint. The resulting defect measured. The
parascapular flap was elevated and the nutrient vessels in the pedicle part were
ascertained. The flap was transplanted in the axillary region. Primary closure of the
donor site was performed. Penrose drain was subcutaneously inserted after adequately
fixing the flap to the base by suturing and the operation was completed.
RESULTS
Thirty five procedures had
been performed to release post-bum axillary scar contractures in 35 patients (Table l):
Type I comprised 10 patients reconstructed by 5-flap Y-V advancement and Z-plasty
procedure (Fig. 2), type II included 20 patients reconstructed by lateral thoracic
pedicled fasciocutaneous flaps in 5 patients (Figs. 3,4) and.inner arm pedicled
fasciocutaneous flaps in 15 patients (Figs. 5,6) and five patients with types III and IV
were reconstructed by parascapular island fasciocutaneous flap (Figs. 7,8). All flaps
survived even when raised in scar tissue or areas previously grafted. Satisfactory release
was obtained in all cases and non of the patients has required a second interference, with
no recurrence of contracture. Splintage was not used after the initial postoperative
period. The average time of hospitalization was 10 days. The maximum period of follow-up
had been 9 months.
| Surgical procedure |
Age
(years) |
Sex |
TBSA burn
(%) |
3rd� burn
(%) |
Time from burn
to release (years) |
Aetiology |
| Male |
Female |
Flame |
Scald |
| Whole group |
15.6�8.7 (4.5-31) |
14 |
21 |
23.3�9.8 (10-40) |
12.5�6.5 (5-25) |
3.3�2.7 (0.5-13) |
25 |
10 |
| 5-flap |
12.9�9.6 (5-30) |
5 |
5 |
23�10.6 (10-40) |
11.4�6.2 (5-25) |
3.3�2.2 (2-8) |
6 |
4 |
| Laterale thoracic pedicled FCF |
10.3�6.3 (4.5-18) |
2 |
3 |
17�5.7 (10-25) |
9.4�5.2 (5-15) |
2.1�2.2 (0.5-4) |
3 |
2 |
| Inner arm pedicled FCF |
17.2�8.7 (5-30) |
6 |
9 |
23.3�9.2 (10-40) |
12.7�6.4 (5-25) |
3.4�3.3 (1-13) |
11 |
4 |
| Parascapular island FCF |
21.2�5.2 (17-30) |
1 |
4 |
30�11.7 (15-40) |
17�7.6 (10-25) |
4.2�2.9 (2-9) |
5 |
- |
|
Table
(1): Patient population |
|
 |
|
Fig (1): Five-flap Y-V advancement
and Z-plasty. |
 |
|
 |
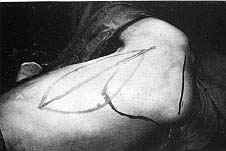
| Fig. (2 - A): Postburn scar contracture of left anterior
axillary fold in a male patient aged 8 years (Type I) reconstructed by five-flaps.
Preoperative |
|
Fig.
(2- B): Postburn scar contracture of left anterior axillary fold in a male
patient aged 8 years (Type I) reconstructed by five-flaps. Post operative view |
 |
|
 |
| Fig.
(3-A): Postburn scar contracture of the left posterior axillary fold in a male
patient aged 8 years (Type II) reconstructed by lateral thoracic pedicled fasciocutaneous
flap.Preoperative |
|
Fig.
(3-B): Postburn scar contracture of the left posterior axillary fold in a male
patient aged 8 years (Type II) reconstructed by lateral thoracic pedicled fasciocutaneous
flap.Postoperative. |
|
 |
|
 |
| Fig.
(4-A): Postburn scar contracture of the left anterior axillary fold in a female
patient aged 4.5 years (Type II) reconstructed by lateral thoracic pedicled
fasciocutaneous flap.Preoperative |
|
Fig.
(4-B): Postburn scar contracture of the left anterior axillary fold in a female
patient aged 4.5 years (Type II) reconstructed by lateral thoracic pedicled
fasciocutaneous flap.Postoperative. |
 |
|
 |
| Fig.
(5-A): Postburn scar contracture of the left anterior axillary fold in a female
patient aged 20 years (Type II) reconstructed by inner arm pedicled fasciocutancous
flap.Preoperative b) Postoperative. |
|
Fig.
(5-B): Postburn scar contracture of the left anterior axillary fold in a female
patient aged 20 years (Type II) reconstructed by inner arm pedicled fasciocutancous
flap.Postoperative. |
 |
|
 |
| Fig.
(6-A): Postburn scar contracture of the left anterior axillary fold in a female
patient aged 22 years (Type II) reconstructed by inner arm pedicled fasciocutancous
flap.Preoperative. |
|
Fig.
(6-B): Postburn scar contracture of the left anterior axillary fold in a female
patient aged 22 years (Type II) reconstructed by inner arm pedicled fasciocutancous
flap.Postoperative. |
 |
|
Fig. (6-C): Postburn scar contracture of the left
anterior axillary fold in a female patient aged 22 years (Type II) reconstructed by inner
arm pedicled fasciocutancous flap.After 6 months. |
|
 |
|
 |
| Fig.
(7-A): Postburn scar contracture of the right axilla (Type IV) in a male patient
aged 20 years reconstructed by parascapular island fasciocutancous flap.Preoperative. |
|
Fig.
(7-B): Postburn scar contracture of the right axilla (Type IV) in a male patient
aged 20 years reconstructed by parascapular island fasciocutancous flap.Flap design. |
 |
|
 |
| Fig.
(7-C): Postburn scar contracture of the right axilla (Type IV) in a male patient
aged 20 years reconstructed by parascapular island fasciocutancous flap.Flap elevation. |
|
Fig.
(7-D): Postburn scar contracture of the right axilla (Type IV) in a male patient
aged 20 years reconstructed by parascapular island fasciocutancous flap.Flap inset. |
 |
|
Fig. (7-E): Postburn scar contracture of the right
axilla (Type IV) in a male patient aged 20 years reconstructed by parascapular island
fasciocutancous flap.Ten days postoperative. |
|
 |
|
 |
| Fig.
(8-A): Postburn scar contracture of the right axilla (Type IV) in a female
patient aged 15 years reconstructed by parascapular island fasciocutaneous
flap.Preoperative |
|
Fig. (8-B): Postburn scar contracture of the right
axilla (Type IV) in a female patient aged 15 years reconstructed by parascapular island
fasciocutaneous flap.Flap design |
 |
|
 |
| Fig. (8-C): Postburn scar contracture of the right
axilla (Type IV) in a female patient aged 15 years reconstructed by parascapular island
fasciocutaneous flap.Flap elevation. |
|
Fig. (8-D): Postburn scar contracture of the right
axilla (Type IV) in a female patient aged 15 years reconstructed by parascapular island
fasciocutaneous flap.Flap inset. |
|
DISCUSSION
The
armamentarium of the reconstructive burn surgeon comprises direct closure, grafts, flaps,
free tissue transfer and tissue expansion [11].The standard method of correcting burn
contractures running across the flexor surfaces of joints or of hollows in the body
surface, is to cross-cut the scar tissue down to underlying normal tissue and to fill the
defect created with a split-skin graft [12].This method has several disadvantages [7]: (1)
The grafted area can recontract. Althoughthe amount can be reduced by the use of a thick
skin graft, this may lower the percentage take of the graft. Some surgeons attempt to put
in an excess of skin so that any further recontracture will take up this skin. This can
have an ugly wrinkled area of graft. (2) Part of the split skin graft can fail to take,
which may result in further surgery or repeated dressings, leading to a delay in healing.
A greater extent of contracture can then occur. (3) In the case of severe burns, there may
be an absence of suitable donor sites to yield a good single sheet of skin graft. (4)
Pocket formation may occur at both ends of the incision. These may be unattractive and
difficult to keep clean. This complication can be reduced by fish-tailing the ends of the
incision. (5) A long hospital stay is involved so that the graft may have the best chance
of taking and for the donor area to heal. (6) The skin graft donor area is painful. This
is a very major problem for patients who need multiple readmissions for contractures in
different parts of the body. (7) Long-term splining, often used to reduce graft
contracture, can be cumbersome, need frequent checking and readjustment and may be
expensive.Some clinicians have felt musculocutaneous flaps, specifically the latissimus
dorsi, might play a role in axillary bum reconstruction. This flap is much too bulky for
the axilla. The pectoralis may or has also been recommended for axillary reconstruction by
Freedlander et al. [13]. Pectoralis flaps can interfere with function of the upper
extremity. Free flaps have been reported for release of axillary burn contractures [14]
but they are not practical on a routine basis.There are many methods of correction of
postburn bridle scars of the axilla which include local rearrangement of the skin.
Z-plasty (two flaps) [15], square flap (three flaps) [16], double Z-plasty (four flaps)
[17], V-Y advancement and Z-plasty (five flaps) [6], six flaps Z-plasty (six flaps) [18],
seven flaps plasty (two half Zplasties and one W-M plasty) [19]. X-plasty [20], propeller
flap [21] and multiple Y-V plasty [22].The single Z-plasty, with its large flaps, is more
prone to transverse tension, necrosis of the tip of a flap and displacement of the
hairbearing skin of the axilla anteriorly over the chest wall. Using double Z-plasty
procedure, one can avoid using large skin flaps, however, the local anatomic area
(hair-bearing skin of the axilla) will be displaced. The use of combination of five-flap
Y-V advancement and Z-plasty will preserve the local anatomic area and will reduce and
diffuse the transverse tension, thereby minimizing circulatory embarassment.With the
introduction of fasciocutaneous flaps by Ponten [23], there are now a number of larger
flaps available in the axillary region which allow primary closure of total axillary
defects. A series of axillary bum contractures released with the latissimus dorsi
fasciocutaneous flap had been reported by Tolhurst [24,25] and confirmed by Achauer et al.
[26]. Depending on the two cutaneous branches of the circumflex scapular artery, the
scapular flap designed horizontally [27,28] and the parascapular flap designed obliquely
[10,29] have been used to correct axillary postbum scar contractures. Maruyama [30] had
used the ascending scapular flap, based on the ascending cutaneous branch of the
circumflex scapular artery, for the repair of axillary burn scar contracture. A small,
regional fasciocutancous flap of the inner arm had been reported by Beasley; Kaplan &
Pearl and Budo et al [8,31,32] as useful for contractures of the anterior axillary fold.
This flap was originally described by Kaplan and Pearl as an axial pattern (arterial) flap
based on the superior ultiar collateral artery [32]. Budo feels that this inner arm flap
is in reality a fasciocutaneous flap (superflap) because the dissection is carried out
proximal to the origin of superior ulnar collateral artery. It is likely that the blood
supply is based on the fascia of the axilla and anterior shoulder [8]. The posterior arm
fasciocutaneous flap supplied by an unnamed but constant branch of the brachial artery had
been described by Elliot et al. [33] in the reconstruction of the axilla. Roberts and
Dickson [7] and Bhattachrya et al. [34] had reported the use of lateral thoracic
fasciocutaneous flap in the reconstruction of postburn axillary scar contracture. The
advantage of the fasciocutaneous flap is the simplicity of its concept. The surgical
dissection may be performed rapidly with great facility, since the subfascial plan is
relatively bloodless [35]. Thin flaps may be chosen that are extremely pliable to permit
easy recontouring of adjacent defects using tissues similar to the original in color,
texture and consistency. Many of these flap procedures may be done on an outpatient basis,
especially if a skin graft can be avoided. No functional disturbance accrues, since muscle
never has to be sacrificed. No special skills or equipment nor extended usurpation of
operating theater time as demanded for microsurgical techniques is needed [29].An
additional asset of the local fasciocutaneous flap specifically relevant to the burned
patient is that a scarred or skin-grafted region itself may be used as part of the donor
site in many cases, since the perforators to the deep fascia usually are found deep in
intermuscular septa and are protected in most superficial burns. Also, even if the donor
site for the flap must be skin grafted, little additional morbidity or aesthetic deformity
is noticed, since all surgery is resticted to the site of injury [7].Unlike skin grafts,
these flaps have a potential for growth with the patient, little risk of recontracture if
properly performed and greater compliance to allow expansion with motion of the
extremities. No cumbersome splints or intensive long-term physical therapy is needed for
the sometimes uncooperative or noncompliant burn patient. Since only a single storage is
required, the need for multiple surgical procedures, such as with tissue expansion, may be
avoided, although the latter is another method that had advocates for local tissue
reconstruction for bum deformities [36].From our study, we recommend the use of five flaps
Y-V advancement and Z-plasty procedure in the reconstruction of type I axillary scar
contractures. For type II axillary scar contructures, either the lateral thoracic pedicled
fasciocutaneous flaps or the inner arm pedicled faselocutaneous flaps is suitable. As
regards types III and IV axially scar contractures we prefer the use of parascapular
island fasciocutaneous flap in their reconstruction as the defect resulting in these cases
is surprisingly large needing a flap with large dimensions.
REFERENCE
- Willis B., Larson D.L. and Abston
S.: Positioning, and splinting the burned patient. J. Heart Lung, 2: 696,1973.
- Burke J.F., Quinby W.C., Behringer G.E. et
al.: Approach to burn therapy. Surg. Ann., 13: 1, 1981.
- Larson D.L., Abston S., Willis B. et al.:
Techniques for decreasing scar formation in the burned patient. J. Trauma, 11: 807,
1971.
- Larson D.K., Abston S., Willis R. et al.:
Contrcture and scar formation in burn patients. Clin. Plast. Surg., 1: 653, 1974.
- Hanumadass M., Kagan R., Matsuda T. and
Jayaram B.: Classification and surgical correction of postburn axillary contractures. J.
Trauma, 26: 236, 1986.
- Hirshowitz B., Karev A. and Levy Y.: A
5-flap procedure for axillary webs leaving the ape?( intact. Br. J. Plast. Surg., 30: 48,
1977.
- Roberts A.H.N. and Dickson W.A.:
Fasciocutaneous flaps for burn reconstruction: a report of 57 flaps. Br. J. Plast. Surg.,
41: 150, 1988.
- Budo J., Finucan T. and Clarke J.: The
inner arm fasciocutaneous flap. Plast. Reconstr. Surg., 73: 629,1984.
- Nassif T.M., Vidal L., Bovet J.L. and
Baudet J.: The parascapular flap: A new cutaneous microsurgical free flap. Plast.
Reconstr. Surg., 69: 591, 1982.
- Yanai A., Nagata S., Hirabayashi S. and
Nakamura N.: Inverted-U parascapular flap for the treatment of axillary burn scar
contracture. Plast. Reconstr. Surg., 76: 126, 1985.
- Robson M.C., Barnett R.A., Leitch LON. and
Hayward P.G.: Prevention and treatment of postburn scars and contracture. World. J. Surg.,
16: 87, 1992.
- Metaizeau J.P., Gayet C., Schmitt M. and
Prevot J.: The use of free full-thickness skin grafts in the treatment of complications of
burns. Progress in Pediatric Surgery, 14: 209, 1981.
- Freedlander E, Lee K. and Vandervord J.G.:
Reconstruction of the axilla with a pectoralis major myocutaneous island flap. Br. J.
Plast. Surg., 35: 144, 1982.
- Ohmori S.: Correction of burn deformities
using free flap transfer. J. Trauma, 22: 104, 1982.
- Bretteville-Jensen G.: Marking the 60�
Z-plasty to achieve accurate lengthening. Br. J. Plast. Surg., 30: 72, 1977.
- Hyakosoku H. and Funifiri M.: The square
flap method. Br. J. Plast. Surg., 40: 40, 1987.
- Woolf R.M. and Broadbent T.R.: The four
flap Z-plasty. Plast. Reconstr. Surg., 49: 48, 1972.
- Mir Y. and Mir L.: The six flap Z-plasty.
Plast. Reconstr. Surg., 52: 625, 1973.
- Karacoaglan N. and Uysal A.: The seven
flapplasty. Br. J. Plast. Surg., 47: 372, 1994.
- Vartak A. and Keswani M.H.: X-plasty for
repair of burn contractures. Burns, 18: 326, 1992.
- Hyakosoku H., Yamamoto T. and Fumiiri M.:
The propeller flap method. Brit. J. Plast. Surg., 44:53,1991.
- Cooper M.A. C.S.: The multiple Y-V plasty
in linear burn scar contracture release. Br. J. Plast. Surg., 43: 145, 1990.
- Ponten B.: The fasciocutaneous flap: Its
use in soft tissue defects for the lower leg. Br. J. Plast. Sur,a., 34: 215, 1981.
- Tolhurst D.E. and Haeseker B.:
Fasciocutaneous flaps in the axillary region. Br. J. Plast. Surg., 35: 430, 1982.
- Tolhurst D.E., Haeseker B. and Zeeman R.J.:
The development of the fasciocutaneous flap and its clinical applications. Plast.
Reconstr. Surg., 71:597,1983.
- Achduer B.M., Spenler CM. and Gold M.E.:
Reconstruction of axillary burn contractures with the latissimus dorsi fasciocutaneous
flap. J. Trauma, 28: 211, 1988.
- Diamond M. and Barwick W.: Treatment of
axillary burn scar contracture using an arterialized scapular island flap. Plast.
Reconstr. Surg., 72: 388, 1983.
- Teot L. and Bosse J.P.: The use of scapular
skin island flaps in the treatment of axillary postburn scar contractures. Br. J Plast.
Surg., 47:108, 1994.
- Hallock G.G.: The role of local
fasciocutaneous flaps in total burn wound management. Plast. Reconstr. Surg., 90: 629,
1992.
- Maruyama Y.: Ascending scapular flap and
its use for the treatment of axillary burn scar contracture. Br. J. Plast. Surg., 44: 97,
1991.
- Beasley R.W.: Burns of axilla and elbow.
In: J.M. Converse (Ed.): Reconstructive Plastic Surgery, 2nd Ed., Vol. 6. Philadelphia:
Saunders. P. 3391, 1977.
- Kaplan E.N. and Pearl R.M.: An arterial
media] arm flap-vascular anatomy and clinical applications. Ann. Plast. Surg., 4: 205,
1980.
- Elliot D., Kangesu L., Bainbridge C. and
Venkataramarkrishnan V.: Reconstruction of the axilla with a posterior arm fasciocutaneous
flap. Br. J. Plast. Surg., 45: 101, 1992.
- Bhattachrya S., Bhagia S.P., Bhatnagar S.K.
and Chandra R.: Lateral thoracic region flap. Br. J. Plast. Surg., 43: 162, 1990.
- Tolhurst D.E.: Fasciocutaneous flaps and
their use in reconstructive surgery. Perspect. Plast. Surg.. 4: 129, 1990.
- Hallock G.G.: Tissue expansion techniques
in burn reconstruction. Ann. Plast. Surg., 18: 271, 1987.
|