 |
Egypt. J. Plast. Reconstr. Surgg.,
Vol. 23, No. 1, 1999: 35 - 40 |
Treatment of Burn Alopecia with
Temporo-Parieto-Occipital Flap
MOHAMAD OSAMA KOTB, M.D.
The Department of Plastic Ahined Maher Teaching Hospital, Cairo.
ABSTRACT
Fifteen cases suffering from burn alopecia were treated
by a temporo-paricto-occipital flap for recreation of the frontal hairline. Flap delay for
10 day was used in 11 cases to augment their blood supply. There were 3 minor post
operative necrosis of the distal 1-2 cm of the flap and the remaining 12 cases had
complete flap survival. The results were discussed and it was concluded that using the
temporo-paricto-occipital flap is a simple, quick and safe procedure to recreate the
anterior hairline in patients with burn alopecia.
INTRODUCTION
Fifteen cases suffering from burn alopecia were treated
by a temporo-paricto-occipital flap for recreation of the frontal hairline. Flap delay for
10 day was used in 11 cases to augment their blood supply. There were 3 minor post
operative necrosis of the distal 1-2 cm of the flap and the remaining 12 cases had
complete flap survival. The results were discussed and it was concluded that using the
temporo-paricto-occipital flap is a simple, quick and safe procedure to recreate the
anterior hairline in patients with burn alopecia.
PATIENTS AND
METHODS
During the last 2 years, the temporo-parietooccipital
flap procedure was used in fifteen patients with postburn alopecia. Nine patients were
males and six were females. Their ages range from 4 to 40 years. The cause of the bum was
flame in 10 patients, scald in 3 and chemical in 2 patients. In 4 of the patients the flap
was raised directly without delay, while the other 11 patients the flap raising was
delayed for 10 days. In 1 patient the flap was raised bilaterally.
Operative techniques:
The temporo-paricto-occipital flap is based on the posterior branch of
the superficial ternporal vessels and their patency can be assessed by doppler
ultrasonography. The flap is outlined preoperatively as is the area of hairless frontal
scalp to be excised.The plane of dissection is between the galea and
the skull pericranium. The haemostasis is best achieved by using Allis forceps or scalp
clips rather than cautery to ensure viability of the flap edges [8]. A delay is frequently
recommended, following the flap raising, it is sutured again to its bedwhere it will be
raised after 10 days and then rotated into the recipient's bed after excision of the
burned area. A subgaleal drain is left for 24 hours to decrease the risk of haematoma. A
dog ear will usually occur at the pedicle base point of rotation. It is adjacent to the
vascular supply of the flap and should be allowed to remain after the procedure is
completed. It will flatten with time and if necessary can be surgically revised after I
year [9].The donor site is closed directly without tension after wide undermining of the
edges. A non pressure dressing is applied, as pressure may compromise blood supply of the
flap. The patient is allowed to shampoo on the second day and the sutures are removed
after 10- 12 days [1].
R ESULT
In this study no total flap loss had occurred
in 16 flaps raised. There were 3 cases in which post operative necrosis at the distal 1-2
cm of the flap, 2 had occurred with undelayed flaps and I condition with a delayed flap
but all 3 were healed by secondary intention. No wound infection or haematoma were seen in
our patients. Table (1) illustrates the data of 15 casesThe length of the flap ranged from
14-20 em, while the flap's width ranged from 2.5-3 em. Flaps measuring 14 to 15 cm never
developed distal necrosis, in contrast to those 16 to 20 em in length. The donor site
healed by primary intention in all patients. Minor alopecia appeared in 3 donor sites post
operatively.
Table (1): Results
of the teinporo-paricto-occipital flap in 15 patients with burn alopecia.
| Case No. |
Sex |
Age (years) |
Flap size (cm) |
Delay |
Flap complications |
Donor site complications |
| 1 |
Female |
15 |
16 x 3 cm |
- |
|
|
| 2 |
Female |
40 |
17 x 3 |
- |
Necrosis of distal 2 cm |
|
| 3 |
Male |
5 |
15 x 2.5R
15 x 2.5L |
-
+ |
Necrosis of distal 1 cm (R. side ) |
|
| 4 |
Male |
6 |
17 x 2.5 |
+ |
|
|
| 5 |
Male |
20 |
16 x 3 |
- |
|
Mild alopecia |
| 6 |
Female |
4 |
14 x 2.5 |
+ |
|
|
| 7 |
Female |
22 |
20 x 3 |
+ |
Necrosis of distal 1.5 cm |
Mild alopecia |
| 8 |
Male |
30 |
16 x 2.5 |
+ |
|
|
| 9 |
Male |
14 |
15 x 3 |
+ |
|
|
| 10 |
Female |
20 |
17 x 2.5 |
+ |
|
|
| 11 |
Male |
10 |
16 x 3 |
+ |
|
|
| 12 |
Female |
8 |
15 x 2.5 |
+ |
|
|
| 13 |
Female |
14 |
15 x 2.5 |
+ |
|
|
| 14 |
Male |
21 |
16 x 3 |
+ |
|
Mild alopecia |
| 15 |
Male |
10 |
15 x 2.5 |
+ |
|
|
| Table (1):
Results of the teinporo-paricto-occipital flap in 15 patients with burn alopecia. |
|
 |
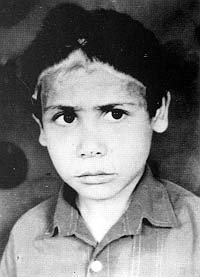 |
| Fig(1):
a-Pre and b- Post operative photographs of case No. 3 |
 |
 |
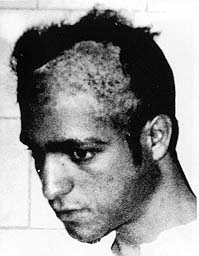
| Fig(2):
a-Pre and b- Post operative photographs of case No. 4 |
 |
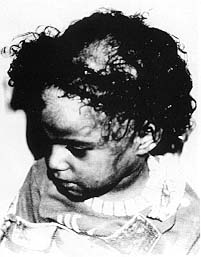 |
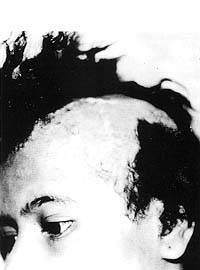
| Fig(3):
a-Pre and b- Post operative photographs of case No. 6 |
 |
 |
| Fig(4):
a-Pre and b- Post operative photographs of case No. 8 |
 |
 |
| Fig(5):
a-Pre and b- Post operative photographs of case No. 10 |
 |
 |
| Fig(6):
a-Pre and b- Post operative photographs of case No. 13 |
|
DISCUSSION
Scalp flaps have been used to reconstruct the
anterior hairline. Dardour et al. [11 used one stage preauricular random flap for male
baldness without a delay and they stated that risk factors were tobacco consumption,
anxiousness, thin flaps and haematoma formation. Rizetto and Ellenbogen [10] reported 62
undelayed temporo-parieto-occipital flaps for male baldness with adequate hair growth in
all patients.In the present study, 15 cases suffering from burn alopecia were treated by
temporo-parietooccipital flap to recreate anterior hairline. Threecases had necrosis at
1-2 cin of the flap distalend, two of them with undelayed flaps and one with a delayed
flap. The other twelve cases had complete viable flaps with accepted post operative
results. The advantages of the temporoparieto-occipital flap procedure are:
- Easy quick operation and short hospital stay.
- High hair density and aesthetic frontal hairline.
- The 2 stages of the operation can be done within 10 days.
- Direct closure of the donor site.
- In severe alopecia it could be the first stage procedure, allowing a
quick pleasant aspect, that would be completed afterwards by scalp reduction, punch grafts
or tissue expansion [11].
The disadvantages of the temporo-parietooccipitalflap procedure are:
- Posterior direction of hair growth.
- Dog ear usually occurs at the pediele base[12].
- Delay procedure causes scarring of the flap edges which may lead to
difficult closure of the donor site.
- Alopecia might occur at the donor site if closure is under significant
tension.
- Necrosis at the distal end of the flap, especially if its length is more
than 17 em, which can be repaired by fusiform graft and the final result is obtained
before 6 months.
In conclusion, the results achieved in this study point out that
temporo-paricto-occipital flap with one delay is a simple, quick and safe procedure for
recreation of the anterior hairline in bum alopecia.
REFERENCE
Dardour J.C., Pugash E. and Aziza
R.: The onestage preauricular nap for male pattern baldness: Long term results and risk
factors. Plast. Reconstr. Surg., 81: 907, 1988.
Nataf J.: Surgical treatment for
frontal baldness. The long temporal vertical flap. Plast. Reconstr.Surg., 74: 628, 1984.
Smith J.W. and Aston S.J.:
Treatment of baldness with the use of flaps-Grabb and Smith's plastic surgery-4th
edition-Little, Brown and Company, p: 635, 1991.
Unger W.: Treatment of bladness.
Grabb and Smith's plastic surgery-5th edition- lippincottRaven publishers, Philadelphia,
p: 569, 1997.
Argenta L.C.: Controlled tissue
expansion in reconstructive surgery. Brit. J. Plast. Surg., 37: 520, 1984.
Frechet R: Scalp extension. J.
Dermatol. Surg.Oncol., 19: 616, 1993.
Juri J.: Use of parieto-occipital
flaps in the surgical treatment of baldness. Plast. Reconstr. Surg., 55:456,1975.
Mathes S. and Nahai F.: Scalp
flap. Reconstructive surgery, Principles, Anatomy and Technique-churchill livingstone.
Vol. 1, 333, 1997.
Huang T.T., Larson D.L. and Lewis
S.R.: Burn alopecia. Plast. Reconstr. Surg., 60: 763, 1977.
Rizatto-Stubel A., Ellenbogen R.:
Male baldness: Immediate single stage rotation of very long arterialized temporo-parieto-
occipital flaps. Plast. Reonstr. Surg., 77: 215, 1986.
Paul Buhrer D., Huang T.T., Yee
H.W & Blackwell S1: Treatment of burn alopecia with tissue expanders in children.
Plast. Reconstr. Surg., 81: 512, 1988.
Lesavoy M.A., Dubrow T.J.,
Schwartz RJ, Wackym P.A., Eisenhauer D.M. and McGuire M.: Management of large scalp
defects with local pedicle flaps. Plast. Reconstr. Surg., 91: 783, 1993,
|