Increasing the Flexibility of Feeding Formulas for Burned Patients: The Design of an Easy Computer Program AMR
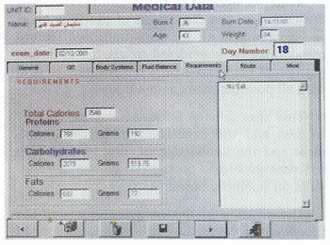
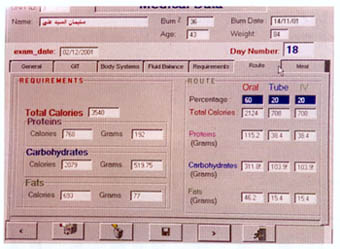
MAGDY, M.D. ABSTRACT The calculation and design of the nutritional requirements for burned patients appear to be somewhat complicated and confusing to personnel in charge in burn units. Many mathematical formulas and input data as well as variables in the medical condition of each patient are to be considered. For easy and accurate calculation of these nutritional needs a computer program is designed and described. Input data include: Patient age, weight, percent of body surface area burned and any associated medical illness or system failure. Depending on calculations using Curreri formula for total caloric needs and Davis and Liljedahl formula for protein needs, the output data includes: The total calories needed and their fragmentation into the three major food categories: carbohydrates, proteins and fats. These are further subdivided over three to four meals and the contents of each meal are listed. The menu of the foodstuff described as well as the route of feeding are changed according to the amount needed and the presence or absence of medical contraindications. This program was used and tested on 40 patients and proved to be easy, accurate and useful in the burn unit. INTRODUCTION Adequate nutritional supply for the burned patient has an important role in patient outcome 111. Estimation of the nutritional needs depends on mathematical formulas for calculating the total caloric and protein needs, according to patient age, weight and surface area burned 12-41. The application of these formulas might be easy, but the design of a complete nutritional protocol appears to be somewhat complicated and time consuming to personnel in charge in the burn units as many difficulties are met with [5]. The presence of organ dysfunction or the development of system failure, during the course of treatment or after resuscitation of a severe injury, represents a dilemma in defining the ratio between the major food fractions: carbohydrates, fats and proteins 161. In these situations, special considerations according to the system affected are to be followed. In many cases with multiple system affection, these considerations might be contradicting to each other and the interpretation of data is perplexing. In this situations, it is difficult to decide which system precaution have the priority to be fulfilled to define the ratio between carbohydrates, fats and proteins 1161. The selection of the routes of administration and the calculation of the relative amounts of the major food fractions to be delivered through each route adds to the difficulties. The final stage of translating these figures into food materials by applying The Food Value Tables [71 to get the daily patient menu according to his daily requirements, is usually the job of the dietitian. But as this is not available in most of our hospitals, the physician carry on this step which is confusing and time consuming. So, there was a need to design a computer program that can accurately calculate these needs and present the results in the form of a daily food menu to be executed directly by the hospital kitchen. This program has to be dynamic so the menu changes according to the changes in the general condition of the patient and even the different foodstuffs described can be also changed according to patient preference. MATERIAL AND METHODS The nutritional needs of 80 patients admitted to Ain Shams University Burn Unit during the years 1999 and 2000 were calculated by the traditional manual techniques according to Ain Shams University Burn Unit nutritional protocol. The total caloric requirements were estimated using Cureri formula [3,41 and the protein needs were calculated using Davis and Liljedhal formula [51. In patients with no organ dysfunction, the carbohydrate to fat ratio was defined as 3:1 181. Patients who had or developed one or more system dysfunction or failure, received the appropriate management and calculations were done depending on their condition following the unit protocol, standard nutritional rules and the current literature [9-171. For example: Patients with renal failure need protein and fat restriction [91 and minimal fluid intake [101. In patients with liver failure, proteins and fats are also restricted [11,121. Carbohydrates, especially parenteral glucose, are limited with relative increase in the ratio of administrated fat, in patients with respiratory failure [131 specially for those who are on ventilators [141. In cases with severe GIT problems the main supply is through the parenteral route [151 and in the presence of heart failure, more fat is used to supply adequate mounts of calories in a reasonable volume [161. This is also the case in patients with large surface area burns [171. All patients were closely observed and their progress was examined clinically and by laboratory investigations. The changes in their nutritional regimen according to systemic changes were documented and analyzed till stabilization of their general condition and stationary progression is achieved. These data were collected and analyzed and used in the design of a computer program. Program design: The flowchart was designed as follow: Step 2: The protein needs are determined, in grams, using Davis and Lilijedhal formula [41. They are adjusted according to the presence or absence of renal [91 or liver [111 impairment and whether the patient is on dialysis [101 or in hepatic coma [121 (Fig. 1). Step 3: the calories derived from the protein needs are obtained and the non protein calories, carbohydrates and fats, are calculated. Step 4: The ratio between carbohydrates and fats are modified according to the medical condition and the state of body systems (Fig. 2). Step 5: The route of feeding and the amounts of calories supplied through each route are defined according to the level of consciousness, whether the patient is on ventilator or not, the gastro-intestinal tract state, the heart condition and the percent of burn (Fig. 3). Step 6: These requirements are translated into either food menus of user selection using Food Value Tables [71 for enteral nutrition, or intravenous prescriptions in case of parenteral nutrition. By the help of a computer specialist, this flow chart was assembled
and translated into an expandable computer program using visual basic
programming tool based on Microsoft Access Database. Its setup
application can be installed on any personal computer with minimal hard
ware requirements: 486 MHz processor, 16 mega bite RAM, Windows 95
operating system and 5 mega bite free space on the hard disc (Fig. 4). The output data are: Total calories needed, the amount of carbohdyrates, fats and protein needed, both in grams and calories, the routes of supply and the relative amount to be delivered through each route (Figs. 9-10). For the selection of the desired food menu, a food preference list is displayed and the user clicks on the desired food item. With the help of a calorie counter, the computer will calculate the amount needed from these foodstuffs to reach the target nutrition and print out the menu (Fig. 1 1). The extra demands of tube and parenteral nutrition are also listed. The program was applied on 40 patients in Ain Shams University Burn
Unit and its accuracy and The time needed for complete nutritional regimen design using the program was estimated and compared to that needed for manual calculations for the same patients. Questionnaire for the personnel working in the unit, twenty doctors and ten nurses, was also performed regarding the ease in using the program, the comfort in data entry and retrieval and the output form. RESULTS The application of the program on patients proved it simplicity, effectiveness in management and accuracy in estimating the nutritional requirements. All the patients had 100% accurate estimates compared to manual calculations. Ninety three percent of patients with no system affection could maintain their body weight within 90% of their pre-burn weight and their laboratory data showed maintenance of the serum protein level and liver functions within acceptable range. Eighty one percent of the patients with serious injuries, or having one or more system affection, could maintain a stationary progress and no nutritional related deterioration in their general condition was observed, for a considerable period of time, indicated by the laboratory data profile relevant to the system affected. The percent of actual calories received by the patients to the target total calories needed was increased from 82% to 91 %. There was a great reduction in time needed for calculating the needs and producing the final food menu than in manual calculations. The average time needed was 5.1±2.8 minutes compared to 21.3±2.5 minutes for complete regimen design in the. first time of patient data entry. This was further reduced to 3.2±1.7 minutes compared to 15±1.8 minutes in subsequent calculation for the same patient. The questionnaire results showed that 90%0 of the users felt comfort in using the program. No difficulty was reported regarding data entry or retrieval. The output form could be easily interpreted and the overall performance of the personnel in the unit was improved.
DISCUSSION In our computer era this indispensable technology has to be widely applied in depth of our field. We should find nontraditional ways to improve performance and solve technical problems. As a computer program for nutritional planing for burned patients was needed to avoid the difficulties that are met with in using the manual calculations, the main target was to create a simple, accurate and flexible software that provides complete nutritional plan and avoids the drawbacks of the manual calculations. In the design of such a program, the most difficult part was the design of the flow chart and how would all the conditions and recommendations be considered to get the optimum nutritional plan and enable the program to deal with all possible medical conditions. This was greatly achieved and the key of success was the experience in burn management and the knowledge of how to deal with different problems during the course of treatment on scientific bases. The creation of this software increased the flexibility of the feeding formulas to be applied in all medical situations and nearly eliminated the incidence of errors. Being dynamic, the calculated nutrients, -their ratio and route, are individualized and can be easily modified according to changes in the state of body systems. The clinical application of the program was successful. The nutritional estimates were accurate. And its use resulted in great reduction and saving of time wasted in the manual calculation of the feeding regimen. This was reflected on the general outcome and performance in the burn unit and effort is directed to rather more care for the patient. The program provides complete daily macro nutritional requirements list divided into four meals of patient choice. They are selected interactively via menu options. This improves the appetite of the patient as he is now able to choose his own food menu with no added burden on the burn unit personnel. The use of the program also avoids the difficulties met with in dealing with food value tables and the generated regimen more accurately approaches the dietary goals than the manual method. In spite of the successful application of the program, some patients developed changes in their general condition. This was not due to nutritional factors, but rather to other incidents, that might occur during the course of burn management and related to the type and severity of the injury. Here the patients needs could be easily adapted to these changes. The users did not find difficulty in dealing
The program has the ability to expand and data fields are left blank for the user to add new foodstuff to be saved in the program food list and used upon patient desire. A similar list is present to add new items for the tube feeding and intravenous nutrition. In the future, the program should be upgraded and new versions are to be developed according to the users' feed back. This might include, fluid balance recomendations, listing the micro nutrient requirements needed, or feed up the computer by the results of laboratory investigations and their interpretation is done by the program rather than checking the affected system item in the check box. Yet, this might be a little pit sophisticated and needs more time for data entery. This program will stimulate the plastic surgeons to develop more software in other fields of plastic surgery and burn management and give them the initiation to be innovative and creative rather than only users of the modern technology. All what they require is to define their needs or problems, analyze them and put the principles for the solutions in a rather systematic manner. Acknowledgement: REFERENCE
|