Local Fascicutaneus Flaps in Managing Post Burn Breast Deformities WAEL
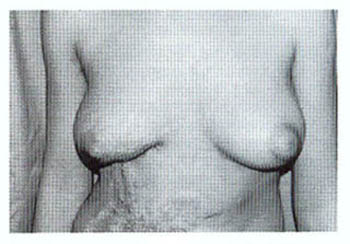
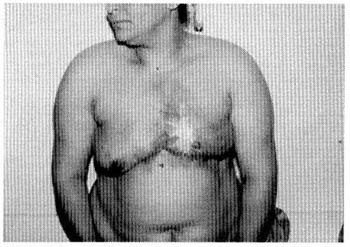
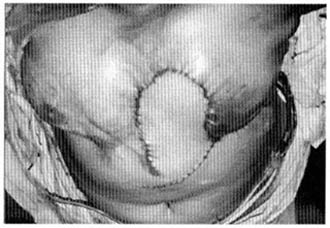
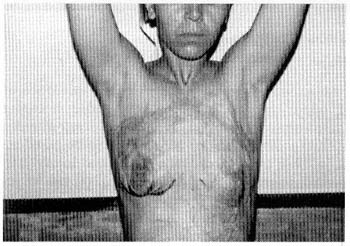
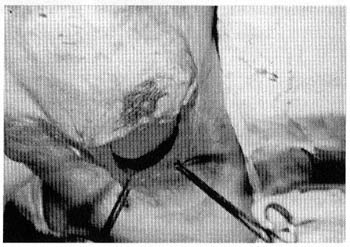
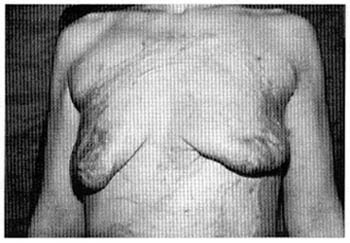
M.R. SAKR, M.D. ABSTRACT During the period from June 1998 to April 2000, thirty-six (36) patients with 40 post-burn breast deformities were operated upon. Patients were divided into 2 groups; the first group (20 deformities) was managed by release and skin grafts. The other group (20 deformities) was managed by release and use of local flaps. Local flaps used were; Z-plasty, local rotation flap, sliding skin flap from the abdominal wall, thoracoepigastric flap and lateral thoracic flap. The results of treatment were evaluated in the early post-operative period and after 6 months. The results were evaluated from the patients and surgeon's point of view. Results showed that the aesthetic and reconstructive outcome was better in group 2 (of release and flap coverage) than in group 1, with little difference in the early post-operative period but with a statistically significant difference between group 1 and group 2 in the late postoperative period. It was concluded that using local flaps is a good option to manage post-burn breast deformities and are superior to using skin grafts especially if breast prosthesis is to be used as a part of management in a later stage. INTRODUCTION The disabilities arising from severe burn injuries have certain unique characteristics not shared by other diseases. Burn patients are more likely to have and remember dramatic circumstances surrounding their injuries. Furthermore, their appearance evokes public avoidance and revolution rather than sympathy [1]. These problems may be further accentuated in female patients with significant deformities of the breast as a result of thermal injury. Far from posing merely cosmetic problem, such deformities deeply disturb both the patient's perception of her body and her emotional balance and they can markedly diminish patient's self esteem and well being [2]. The patient with a breast deformity presents the reconstructive surgeon with a special opportunity and challenge: the opportunity to restore her emotional health and sense of well being and the challenge to create an aesthetically pleasing breast. To achieve the proper results for each patient, there are a myriad of surgical procedures for modification and reconstruction of the breast deformities [3]. Burns of the anterior chest can cause significant distortion to the developing breast. Whenever the breast analogue has been damaged, varying degrees of maldevelopment may occur. However, most authors believe that the breast bud is rarely totally damaged by the burn trauma itself. Loss or distortion of the areola and nipple complex, does not necessarily indicate that the underlying gland will not develop nor that lactation will not occur after pregnancy [4]. There are many indications to operate and repair post-burn breast deformities. Burns to the anterior chest can cause significant distortion to the developing breast abnormal breast development can result from regional scar formation distorting skin position, leading to abnormal breast location. Complete coverage of the breast by hypertrophic scar can prevent expansion of the developing breast mound by direct pressure. In addition, anterior axillary contractures and neck contractures can contract the breast mound laterally and/or superiorly. Burn to the breast can also lead to loss or distortion of the areola and nipple complex and loss of the inframammary fold. A wide range of procedures has been described to deal with these problems. The described techniques involved; scar excision, release and skin grafts, skin graft with post-operative splint or a silicone conformer, single or multistaged skin flaps from chest or abdominal wall, latissimus dorsi myocutaneous flap with or without implant, expanders and implants [5]. In this study local fasciocutaneous flaps were used from a neighboring region where tissue is plentiful, to reconstruct the burned breast skin where the tissue is insufficient, scarred and/or damaged. Most of the techniques had been originally described for post-mastectomy breast reconstruction, but also it could be applied to reconstruction of post-burn breast deformities as indicated. Most of the patients included in the present study suffered moderate or severe form of deformity according to Rubin classification of post-burn breast deformity [6]. Another classification proposed by Kadry et al. [7], where breast scars were classified into: breast to axilla, breast to abdomen and finally breast to breast scars and contractures can be also applied. They preferred surgery in early puberty to avoid restriction of mammary growth. MATERIAL AND METHODS During the period from June 1998 to April 2000, thirty six (36) patients with post burn breast deformities were admitted to the plastic and reconstructive section in Kasr El-Aini Hospitals. The age of the patients ranged from 16 to 48 years. Those patients were having 40 breast deformities, four patients were having bilateral breast deformities. They were studied as regards the following items: history taking, thorough general examination and local examination. In this study the median age of burn injury is 12.16 years old and the median age of operative intervention is 24.6 years old. Patients were randomly divided into 2 groups the first group (20 deformities) was managed by release and skin grafts; the second group (20 deformities) was managed by release and use of local flaps to cover. Local flaps used were Z-plasty, local rotational flap, sliding skin flap from the abdomen, thoracoepigastric flap and lateral thoracic flap. The early and late postoperative results were evaluated; the patients were asked directly about their opinion of the result of the operation, immediately postoperative and after six months aided by their pre-operative photographs. The results were graded as excellent, good, fair and poor. The operating surgeon also evaluated the results retrospectively by review of photographs, with evaluation of symmetry, inframammary line, projection, ptosis and scarring. For each unit there is a score from 1 to 4 points. The results were considered as: During the study period 40 breast deformities were reconstructed, 20 of them by release and graft and the other 20 by release and use of local flaps. The local flaps used were Z plasty (3 cases), rotational flap (2 cases), thoracoepigastric flap (4 cases) and sliding skin flap from the abdominal wall (8 cases), lateral thoracic flap (3 cases). Tissue expansion was added in one case from the group of sliding skin flap of the abdominal wall to give more tissues to use. Finally the results of treatment in the early postoperative period and after 6 months were evaluated in order to reach a certain concept as regard the most appropriate treatment. It is also to have the patient's response and satisfaction in the 2 groups of management. In group 1 nonmeshed thick split thickness skin graft for coverage after release was used. In group 2 local fasciocutaneous flaps were used to cover. Z plasty was used to reconstruct a web on the medial side or the axilla. Rotational flap was used if it can cover the defect without any shifting of the breast. Thoracoepigastric flap has an axial blood supply by means of the lateral branch of the superior epigastric artery. A scar should not destroy the expected site of the artery; a Doppler probe can also detect it. The donor site scar can reach the patient's back up to 10 cm from the midline and is mostly hidden by the brassiere straps. The average size of the flap has been 8X16 cm, but the base has varied from 6 to 12 cm and the length from 12 to 22 cm. In raising the flap, care is taken to include the underlying fascia [9] (Fig. 1). Sliding skin flap from the abdomen is based inferiorly at a level that allows the tissue to be brought upward onto the chest wall according to the need. It depends on a broad blood supply not a single vessel, from the two intricate networks of arteries that supply the anterior abdominal wall. This flap has given excellent results and has two advantages, first it builds up the inframammary line if it is lost as a sequel of burn. The second advantage is stretching the overlying skin over the fixed inframammary fold slowly, resulting in improvement over a period of 6 months with some ptosis as well as tear drop appearance of the reconstructed breast [10]. Lateral thoracic flap is a fasciocutaneous flap located between the axilla and fifth to seventh intercostal spaces in its vertical axis and between the anterior edge of latissimus dorsi and the lateral edge of pectoralis major in its horizontal axis, the skin territory is about 12X8 cm. It is used to cover deformities on the lateral aspect of the breast. The vascular anatomy of this flap is variable by three axial vessels; these include the cutaneous branch of the lateral thoracic artery, the accessory lateral thoracic artery, the cutaneous branch of the thoracodorsal artery. Also, the advantage of the last three flaps is giving a good amount of skin for breast reconstruction so that an implant can be inserted to help in breast reconstruction if needed, either immediately or at a later stage (Fig. 2). RESULTS Our results were evaluated in terms of the final reconstructive and aesthetic outcome, for patients and surgeons. The results were also evaluated in terns of the complications (early and late). Table (2) shows the overall aesthetic results for patients in the two groups, group 1 of release and graft and group 2 of release and different fasciocutaneous flap coverage. Table (3) shows the overall aesthetic results from the surgeons point of view, in which we add 5 items of difference between the pre and post-operative photos. These 5 items are symmetry, level of inframammary line, projection, ptosis and scarring. From these two Tables it can be noticed that the results in group 2 (release and flap coverage) are far better than in group 1, with little difference in the early post-operative results. But the late post-operative results show a statistically significant difference between group 1 and group 2 from the patients' point of view and the surgeon's point of view. Table (4) shows the complications in both groups.
DISCUSSION The female breast is regarded as a symbol of femininity and it plays a decisive role in a woman's sense of physical and emotional vitality. Deviation from normal size, shape, colour, texture and symmetry are interpreted as unattractive. Far from posing merely a cosmetic problem, such deviations deeply disturb the patient's perception of her body and her emotional balance and they can markedly diminish patient self-esteem and well being. The deformed breast already represents a serious aesthetic impairment for the patient. Which can result in corresponding emotional trauma. Surgical intervention may therefore be indicated for aesthetic and emotional reasons, which may often overlap [2]. Although there are a myriad of surgical procedures for modification and reconstruction of the breast deformities and because reconstruction of a breast is an elective procedure, safety should be kept uppermost in the surgeons's mind [3]. In the present study the median age of burn injury is 12.16 y old. Twenty cases (20) were burned at the age of 1-10 years old, 16 cases were burned at an older age group. These data may lead to the possibility that suitable legislation and education will reduce the incidence of scalds to children especially those resulting from hot bath water. Lack of education and a low economic status are thought to be associated with a high incidence of thermal injury [11]. In a study done by Kunert et al. [4] on 39 female patients they performed release and skin grafts in 18 breasts and used myocutaneous flaps in 22 breasts and Z-plasty in 8 breasts and breast reduction in 10 breasts. From this study and other studies in the literature the most common procedures done for post-burn breast reconstruction is release and grafts. In our study results of using all types of local flaps were compared with the results of using skin grafts from both the patient's and the surgeon's point of view. The results showed how much the local flaps are superior to using skin grafts with a statistically significant difference especially in the late post-operative result. Skin grafts had the disadvantages of poor quality of scar tissue and bad colour matching with the rest of the breast skin. Also, in all cases there is post-burn contracted scar of the breast obliterating the inframammary line and lateral projection of the breast, skin graft is not a proper solution to give good projection of the breast. After using skin grafts, loss of skin elasticity and adaptation for expansion was a constant finding. Local flaps give better colour matching and better determination of the inframammary fold when it is lost. Also, using local flaps is better than skin grafts as regards the projection and proper breast contour. Some of these local flaps can be firstly expanded so they can give us more tissues to use in reconstruction. After using these local flaps there is the advantage of possible insertion of breast implant for reconstruction later on, especially if there is breast atrophy secondary to the burn. Conclusion: The local fasciocutaneous flaps is a good option in dealing with post-burn breast deformities from the patient's and the surgeon's point of view. They give better results and fewer complications. Also, they can be considered as a first choice if there is breast atrophy and a breast implant will be inserted later on. REFERENCE
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||