 |
Egypt.
J. Plast. Reconstr. Surg., Vol. 27, No. 1, 2003: 109 - 112 | Experience
with Finger Joint Arthrodesis for the Management of Stiff Post Burn Deformities
MOHAMED KHALED HASSAN,
M.D.
The Departments of Plastic Surgery, Faculty of Medicine,Ain Shams
University.
ABSTRACT
Surgical procedures to correct post burn deformities of the hands and fingers present a special challenge because of the poor quality of the soft tissue coverage. The decreased vascularity of the scarred soft tissue does not allow wide dissection and stripping of tissues. Also, the insertion of plates and screws for fixation is limited due to the tightness of scarred tissues. Different techniques for arthrodesis of finger joints that are successfully used for other conditions may not be quite suitable for treating post burn deformities. Single or double Kirschner Wire (KWire) fixation is a suitably rapid method for bone fixation commonly used during reimplantation of amputated digits. Our experience in finger reimplantation over the past twelve years, showed around fifteen per cent of bony rnalposition in the form of deviation, rotation or angulation. The elective surgery for correction of fixed deformities of fingers by arthrodesis necessitates a more sophisticated technique. In nine patients with post burn fixed flexion deformity of the finger joints, a total number of twenty-two fingers was operated upon for arthrodesis of the proximal interphalangeal joints (PIPJ) to attain a position of function using a single longitudinal K-Wire fixation supplemented by a transverse interosseous wire loop. No major complications were reported in all cases. Postoperative follow-up period extended up to fourteen months. The technique and its advantages are discussed in this article.
INTRODUCTION
Arthrodesis of finger joints and osteosynthesis of amputated digits during reimplantation or fractures are almost similar procedures. Arthrodesis is an elective procedure and time factor is not as critical as in case of reimplantation.
In cases of reimplantation, the amputated part is used to be fixed by a single longitudinal K-Wire or two obliquely crossed K-Wires 111. This is a rapid and fairly suitable procedure for reimplantation but is not perfect as we found that it resulted in around fifteen per cent rate of malposition such as rotation, deviation or angulation of the reimplanted finger or phalanx.
Post burn stiff finger joint is by far the most common indication for arthrodesis in our country. Other less common indications include posttraumatic and post inflammatory stiffness, rheumatoid arthritis and joint pain and/or instability.
Finger joint arthrodesis is an established procedure and many techniques have been described with good results. These techniques include: "Cup and Cone" arrangement with KWire fixation [l,2], interosseous wire fixation [3,4], crossed interosseous wires [5], single loop interosseous wire and K-wire [3], AO internal fixation [6], external fixators [7], tension band arthrodesis [8,9] and dynamic external compression [10].
Using these techniques, complete fusion was reported in 83%-100/0 [3,6,9,101. Yet some of these procedures are quite complex and lengthy and sometimes may jeopardize the vulnerable vascularity of an already scarred soft tissue or osteoporotic
bones.
SUBJECTS AND
METHODS
Nine patients, three females and six males with age ranging from nine. to thirty-five years were operated upon. All patients had post burn fixed flexion deformity of the proximal interphalangeal joints (PIPJ). A total number of twenty-two fingers were operated upon in the past four years. Operative time averaged to twenty-five minutes per finger. The shortest follow up was four months and the longest follow up was fourteen months. No thumbs were affected in these patients and in all patients the metacarpophalangeal joints (MPJ) were mobile. A broad-spectrum antibiotic is given one hour
before operation-to reach tissue effective concentration before tourniquet application-and a second dose to be given twelve hours after operation.
All operative procedures were done under tourniquet control. Exposure of the PIPJ was done through a midline longitudinal dorsal incision. In all cases soft tissue coverage was a scar tissue. Incision was done down to bone and joint capsule, no superficial undermining was done. Instead gentle periosteal elevation was done to minimize soft tissue devascularization as much as possible. It was easier and faster to place a transverse drill hole on each side of the joint before doing the osteotomy while the two phalanges are still fixed together. A suitable stainless steel wire is passed through the holes and the loop is left open without twisting till a later stage. The wire was passed in a direction so as to place the knot on the non-contact surface of the finger; i.e. the ulnar side of the index, middle and the ring finger and the radial side of the little finger. The joint capsule was then incised and the fibrosed lateral ligaments divided. If there were remnants of articular
cartilage it was removed by a knife. The distal end of the proximal phalanx was shaped to a cone, the proximal end of the middle phalanx was shaped into a cup. The removed bone pieces and particles were kept in saline-soaked gauze in case they are needed as filling bone grafts. After conforming the cup and the cone, a KWire was passed in a retrograde direction through the distal joint surface to project through the distal angle of the wound. The joint angle and alignment are then adjusted and the wire is passed in an ante grade direction through the plane of the joint back to the proximal phalanx. The angle of the PIPJ is determined as advocated by Weiland
[11]. To be around forty degrees for the index and increasing by 5 degrees for each finger as we go to the ulnar side. At this stage the need for a bone graft to fill small gaps in the contact area between the two bones is judged. Small fragments removed from the bone ends can be used effectively. The bone chip is inserted into the gap then the interosseous wire is tightened. In three fingers in this series small bone grafts were used to fill small defects in the cup and cone arrangement. Tightening of the interosseous wire will exert a compression force along the axis of the K-wire, this will help to fix the graft in place and prevent rotation along this axis. Skin
closure was done using 5/0 nylon sutures. Aluminum finger splints over the affected finger(s) were applied for two weeks. Routinely, X-ray was done at six weeks postoperatively and the K-wire removed at eight weeks.
All wounds healed by primary intention and no wound or pin tract infection occurred. In all cases clinical bony union was confirmed after wire removal at eight weeks despite six weeks X-ray showed no signs of bony union. There was ulnar drift in one finger (index) but it was around twelve degrees. It did not hinder movement and patient did not ask for revision. One revision was done under local anesthesia (six months postoperatively) to remove an interosseous wire that its knot was wrongfully placed on the radial side of an index finger.
|
|
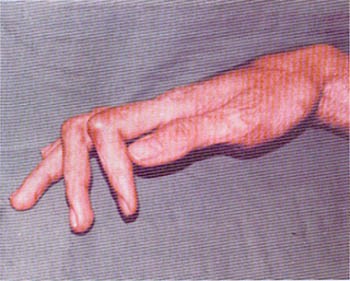
| Fig. (1-A): Post-burn stiff PIP
of the right index and middle fingers of 18 years old male
patient (case-1). |
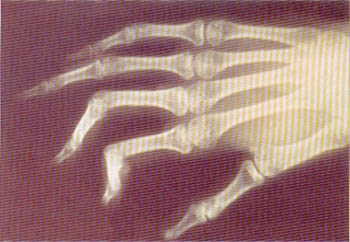
Fig. (1-B): Pre-operative X-ray
showing stiff joints. |
|
|
|
|
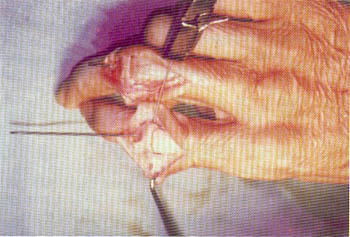
Fig. (1-C): Intra-operative view showing
good bony contact using a cup-and-cone technique fixed by a
combination of K-wire and wire loop. |
Fig. (1-D): Post operative X-ray showing
stiff joints. |
|
|
|
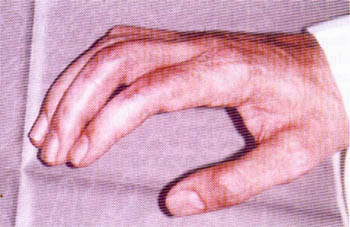
| Fig. (1-E): Early post-operative
view. |
Fig. (1-F): Late post-operative
view. |
|
|
|
| Fig. (2-A): Post-burn stiff PIPJ
of the left index, middle, ring and little fingers of 9 years
old female patient (case-2) |
Fig. (2-B): Post-operative view
of case-2 |
|
|
RESULTS AND DISCUSSION
The most popularly used methods of finger joint arthrodesis are fixation with single or double K-Wire, single or double interosseous wire loops, tension band arthrodesis, plate and screws fixation with or without dynamic compression.
Post burn stiff finger joints is the most common indication for arthrodesis in my practice. These cases present a special challenge among other cases needing arthrodesis because the soft tissue coverage is usually a tight, thin scar with compromised vascularity. This may not allow neither extensive soft tissue dissection for applying tension band fixation; nor the insertion of plates and screws that may protrude through the scarred tissue.
The use of K-wire and/or interosseous wire fixation does not require extensive exposure that may jeopardize soft tissue and bone vascularity. Also, interosseous wire used could be of small gauge that is easily malleable and does not cause problems such as pressure on tight, thin scars or protrusion and exposure.
By combining a single'K-wire with a single loop of small gauge interosseous wire the following disadvantages could be
avoided:
- A single K-wire may not be sufficient to prevent axial rotation.
- Double K-wires may cause distraction at the fracture site.
- A single interosseous loop may not be sufficient to keep the desired angulation.
- The disadvantage of double interosseous loops is that 2 knots are to be placed, the vertical one can not be place dorsally especially if skin is very thin or scarred as in most of the post burn cases. Also, to place it on the volar side more dissection is required and this may adversely affects an already marginal blood supply.
Also, by using this combination, a cup-andcone arrangement can be effectively established with the following
advantages:
- It allows wider surface of bone contact.
- The two bones can be easily manipulated and adjusted than in flat osteotomies.
By using a single K-Wire supplemented by an interosseous wire loop a hundred per cent clinical bony union was achieved with only less than 5% unfavorable result (a single case with ulnar drift) which indeed could be avoided with more technical care. This method of arthrodesis is a very reliable and reproducible technique and could be considered as method of choice in cases of post burn
deformities.
REFERENCE
- Carroll R.E. and Hill N.A.: Small joint arthrodesis in hand reconstruction. J. Bone Joint Surg., 51 A: 1219, 1969.
- 2- Hill N.A.: Small joint arthrodesis. In Green D.P. (Ed): Operative hand Surgery. Vol. l p 113. Edinburgh, Churchill Livingstone, 1982.
- Lister G.: Intraosseous wiring of the digital skeleton. J. Hand Surg., 3: 427, 1978.
- Hogh J. and Jensen P.: Compression-arthrodesis of finger joints using kirschner wires and cerclage. Hand, 14:149, 1982.
- Vanik R.K., Weber R.C., Matloub H.S., Sanger J.R. and Gingrass R.P.: The comparative strengths of internal fixation techniques. J. Hand Surg., 9A: 216, 1984.
- Wright C.S. and McMurty R.Y.: AO arthrodesis in the hand. J. Hand Surg., 8: 932, 1983.
- Tupper JW.: A compression arthrodesis device for small joints of the hands. Hand, 4: 62, 1972.
- Allende B.T. and Engelem J.C.: Tension band arthrodesis in the finger joints. J. Hand Surg., 5: 269, 1980.
- Uhl R.L. and Schneider L.H.: Tension band arthrodesis of finger joints: a retrospective review of 76 consecutive cases. J. Hand Surg. (Am), 17 (3): 518-22, 1992.
- Wexler M.R., Rousso M. and Weinberg H.: Arthrodesis of finger joints by dynamic external compression using dorsoventral kirschner wires and rubber bands. Plast. Reconstr. Surg., 60 (6): 882-5, 1977.
- Weiland A.J.: Small joint arthrodesis and bony defect reconstruction. Chapter in McCarthy J.G., Plastic Surgery Vol. 7 (the hand: edited by May J.W. Jr. and Littler J.W.) pp 4671-4694. Saunders Company, 1990.
|