 |
Egypt.
J. Plast. Reconstr. Surg., Vol. 27, No. 1, 2003: 95 - 99 | Evaluation
of the Role of Dermabrasion and Thin Skin Grafting in the Treatment of
Burn Scar Depigmentation
MAGDY M. DEGHEIDY, M.D.*; IMAN H. EL-MORSY, M.D. ** and KHALID EL-MULLA,
M.D.**
The Departments of Plastic & Reconstructive Surgery* and
Dermatology**, Faculty of medicine, Alexandria University.
ABSTRACT
The study was carried out for 25 patients suffering from post-burn depigmented scars on different sites of their bodies especially on the extremities. Most of cases showed slight surlace irregularities of the depigmented areas. Cases were treated by dermabrasion and thin-splitthickness skin graft application. The technique, advantages, disadvantages and results were discussed. Adequate repigmentation and flat surfaces were obtained in all patients at the end of 6
months.
INTRODUCTION
Normal skin color is dependent on haemoglobin (in both the oxygenated and reduced state), carotenoids and melanin pigments. The major color determinant is melanin and racial and ethnic differences in skin color are related to the number, size, shape, distribution and degradation of melanin-laden organelles called melanosomes. These are produced by the melanocytes and are transferred to the surrounding epidermal keratinocytes [1].
Permanent depigmentation occasionally develops after deep partial-thickness and full thickness burn injuries, which heal by secondary intention. Depigmentation, which is also referred as leukoderma, can cause severe aesthetic problems, particularly in dark-skinned individuals.
The patho-physiology of post-burn depigmentation remains obscure. Studies investigating changes in pigmentation of excisional wounds suggest that scar tissue provides a barrier to melanocyte migration and melanin transfer [2-4].
Medications aiming at stimulation of migration or regeneration of melanocytes along with enhancing melanin production from these melanocytes, proved to be ineffective in treating post burn depigmentation. Different surgical procedures were described aiming at autotransfer of melanocytes to the site of post-burn depigmentation after creation of raw surface by surgical excising or dermabrasion at these sites of depigmentation. Dermabrasion is the preferred method of creating raw surfaces and this can be done by motor driver dermabrader or carbon dioxide laser
[5-10].
MATERIAL AND
METHODS
25 patients suffering from post-burn depigmented scars on different sites of their bodies were the materials of our study. After history taking, clinical examination and laboratory investigations, the depigmented areas were widely abraded with a motor-driven dermabrader.
The abrasion should be deep enough to cause dermal bleeding and to produce a wound surface that is smooth and flat. A thin split thickness skin graft (less than 0-3 mm in thickness) was harvested from the gluteal region, applied over the abraded raw surface and fixed by fine 6/0 sutures. The graft was then covered by a bolus of tie over dressing. The wound was immobilized for a period of a week, the donor site was covered with non-adhesive gauze dressing and pressure was applied with a bandage. The skin graft was exposed after a week where the stitches were removed along with the excess skin graft. Patients were advised to protect their operation sites from sun for at least 3 months and to use skin moisturizers (Figs. 1-5).
Histological examination with silver staining was performed for 5 patients from the depigmented scar tissue and from the skin graft 6 months after its application
(Figs. 6-9).
RESULTS
Out of 25 patients 10 were males and 15 females. Their ages ranged from 18 to 39 years.
All of the operations were successful with excellent to good color matching in most cases. Complications were minimal as shown in Table
(2).
Late post operative (6 months) appearance of the skin graft with excellent color matching.
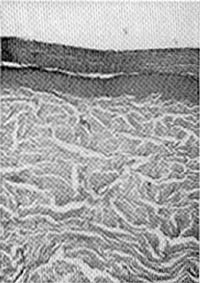
Histological examination of the depigmented scar tissue (Silver stain) showing loss of the normal arrangement of the epidermal layers, loss of the pigmented basal layer and
hyperkeratosis.
Histological examination of the skin graft 6 months after its application showing normal arrangement of the epidermal layer and preservation of the pigmented basal layer.
Histological findings:
Histological examination of the depigmented scar tissue using the silver stain showed loss of
the normal arrangement of the epidermal layers as well as loss of the pigmented basal layer and .hyperkeratosis (Figs. 6,7).
Histological examination of the same area after application of the skin graft (6 months post-operative) using the same silver stain showed normal arrangement of the epidermal layers, preservation of the pigmented basal cell layer
(Figs. 8-9).
| |
No. of patients |
% |
| *Cause of burn |
|
|
| Flame |
13 |
52 |
| Scaled |
8 |
32 |
| Flash |
4 |
16 |
| Total |
25 |
100 |
| *Site of lesion |
|
|
| Extremities |
17 |
68 |
| Face |
5 |
20 |
| Neck |
3 |
12 |
| Total |
25 |
100 |
|
| Table (1): Cause and distribution of burn scars. |
| Complications |
No. of patient |
% |
| Partial skin graft loss due to
haematoma |
1 |
4 |
| Hypertrophic scarring around the
skin graft |
3 |
12 |
| Hyperpigmentation of the skin graft |
3 |
12 |
|
| Table (2): Complications of the procedure. |
|
|
|
| Fig. (1): Post burn scarring of the left forearm
with depigmentation and surface irregurality |
Fig. (2): Dermaabrasion of the scar tissue |
|
|
|
| Fig. (3): Application of the skin graft to the
raw surface after dermabrasion. |
Fig. (4): One week later with excellent take of
the skin graft. |
|
|
|
| Fig. (5): Late post operative (6 month)
appearence of the skin graft with excellent color matching. |
Fig. (6): Low power magnification |
|
|
|
| Fig. (7): High power magnification. |
Fig.(8): Low power magnification. |
|
|
|
|
Fig. (9): High power magnification. |
|
|
DISCUSSION
Depigmented post-burn scar tissue is always resistant to conservative treatment aiming at restoration of its pigment. Autotransfer of melanocytes along with skin grafts to the depigmented area after creation of raw surface seems to be the logical treatment to the problem of depigmented scars
Surgical excision of the depigmented area and skin grafting is considered unfavorable because of dissimilarity in thickness between the graft and surrounding skin
[9].
Dermabrasion is the preferred method of creating raw surface. Mechanical dermabrasion is done by a motor-driver dermabrader and abrasion should be deep enough to cause even dermal bleeding. The great advantage of this procedure is that it leaves a completely viable dermis that binds well with the skin graft [6].
On the other hand, carbon dioxide laser has been used for skin de-epithelization with the great advantage of being very rapid in action with minimal haemorrhage. There is a layer of thermal damage to the remaining dermis which should be very minimal to allow taking of the skin graft. If too much thermal damage remains, skin graft take is affected [l0].
Acikel and Ulkur [11] used C02 laser for dermabrasion of twenty patients with post burn leukodermia and demonstrated a varying amount of thermal damage zone in the remaining dermis. Skin graft loss was demonstrated in 18% of cases. In our study partial skin graft loss was reported in 4% of cases only due to haematoma under the graft.
Selmanowits [12] created raw surfaces in post burn depigmented areas and applied multiple mini grafts. The method is based on the presumed ability of melanocytes to migrate centrifugally from grafts. In our leukoderma patients, we created regular surfaces with mechanical dermabrasion and simultaneously applied very thin skin graft to the depigmented area. There
are many advantages of this procedure compared to the previous method of mini grafting. The preparation and application of the sin graft are much easier and faster and the final scars on the recipient area always appear smooth and normally pigmented even during the very early post-operative period.
Donor-site disability and disfigurement were absent in our study. Post-operative hypertrophic scarring around the graft and skin graft hyperpigentation were reported in 12% of our cases. Erol and Ataby
[15] reported that post-operative skin graft hyperpigmentation was in 5% of their patients only. The higher incidence of skin graft hyperpigmentation in our study can be explained by early excessive exposure of the patients to the sun-rays. On the other hand, hypertrophic scarring around the skin graft can be explained by the racial predisposition to this type of complication among our people.
It is concluded from our study that mechanical dermabrasion and simultaneous thin skin grafting is the treatment of choice for patients with post burn leukoderma, skin graft hyperpigmentation may be avoided by long term sun protection after the operation.
Pressure garments or silicone sheet application is of value in protecting the development of hypertrophic scarring around the skin graft in susceptible
patients.
REFERENCE
-
Jimbow K. and Quevedo W.: Some aspects of melanin biology. J. Invest Dermatol., 67: 72-89,
1976
-
Crikelair G. and Cosman B.: Scars and keloids. Plast Reconstr. Surg., 13: 107-10, 1978.
-
Kalvs S.: Pigment transfer in mammalion epidermis. Arch. Dermatol., 100: 756-62, 1979.
-
Billingham R. and Silvers W.: Studies on the migratory behavior of melanocytes in guinea pig skin. J. EXP Med., 131: 101, 1990.
-
Kahn A. and Cohen M.: Treatment of depigmentation resulting from burn injuries. J. Burn Care Rehab., 22: 552-9, 1996.
-
Erol O. and Atabay K.: The treatment of burn scar hypopigmentation and surface irregularity by dermabrasion and thin skin gaffing. Plast. Reconst. Surg., 85: 754-8, 1990.
-
Taki T. and Izawa Y.: Surgical treatment of skin depigmentation caused by burn injuries, J. Dean Surg. Once]., 11: 12.8-75, 1985.
-
Harashina T. and Iso R.: The treatment of leukoderma after burns by a combination of dermabrasion and chip skin grafting, Br. J. Plast. Surg., 38: 301-8, 1985.
-
Kahn A. and Cohen M.: Treatment of depigmentation following burn injuries. Burns, 77: 552-9, 1996.
-
Hallock G. and Rice D.: Skin deepithelization using carbon dioxide laser. Ann. Plast. Surg., 18: 283-8, 1988.
-
Acikel C. and Ulkur E.: Treatment ol~ burn scar depigmeDtation by carbon dioxide laser-assisted dennabrasion and thin skin grafting. Plast. Reconst. Surg., 95: 1973-8,2000.
-
Selmanowitz V.: Pigmentary correction of Pie baldism by auto grafts. Cutis, 24: 66-75, 1979.
|