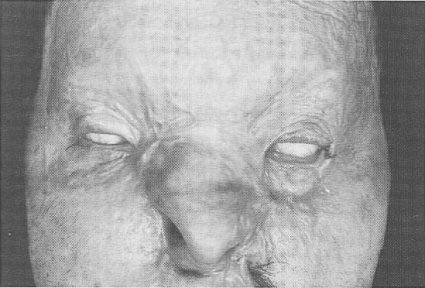
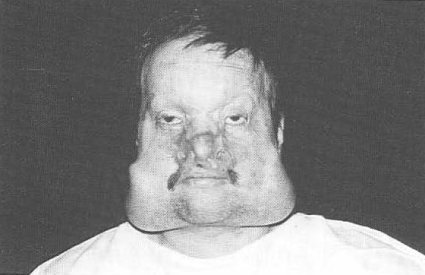
FACIAL BURN SEQUELAE AND TISSUE EXPANSION Although highly. specialised burn centers have significantly reduced mortality. rates following extensive total body surface area burns, survivors are often left with grotesque facial disfigurement. Hypertrophic scars and tissue defects are the most common cause of functional and aesthetic problems in the head and neck region. Plastic surgeons use full-thickness or split-thickness skin grafts, pedicled flaps, free flaps, transplantation of bone or cartilage and tissue expansion. The authors present a case of a patient who suffered from third-degree flame burns to the face. Prior skin grafting procedures left him with severe scar deformity of the face. The patient was treated utilizing multiple tissue expansion. Facial animation has retained and facial integrity has been aesthetically restored and, with the use of make-up, it is near normal in social settings at conversational distances. The tissue expansion technique is advantageous in facial reconstruction because it makes it possible to resurface even wider defects with neighboring skin, similar in colour and texture, and superior to skin obtained elsewhere. The expansion of specialized burn centers has significantly lowered mortality rates in patients with greater than 50% of Total Body Surface Area (T.B.S.A) burns. Many of these burn victims suffer long-term morbidity as a result of functional impairment and grotesque facial appearance (Demling 1989). Facial soft tissue reconstruction is usually one of the most challenging regions for plastic surgeons. This is not only because it usually requires a large amount of soft tissue, but also because of the demand for high quality tissue for its appearance. The optimal goal of the successfully integrated facial reconstruction is characterized by (1) aesthetic balance and symmetry, (2) distinct facial planes, (3) a "doughy" skin texture appropriate for camouflage, and (4j facial animation. In order to achieve these objectives, z-plastics, local flaps, scar releases with full-thickness skin grafts. "pre-patterned" microvascular flaps, extensive intraoperative sculpting of facial contours, hightech computer imaging and cosmetic camouflage techniques are used. Even in optimal circumstances, however, these will never mimic the normal skin perfectly (Feldman 1987) and they often yield "flat", adynamic faces with corrugated, thick surface texture. Even though the cosmetic improvement is an important parameter of overall rehabilitation, too often functional corrections are primarily focused on andaesthetic concerns are relegated to the lowest levels of priority. Tissue expansion has brought about a revolution in soft tissue reconstruction (Masser 1990). Expansion of adjacent skin leads to a flap which matches the area of reconstruction in texture, colour, thickness and sensation (Antony-shyn 1988, Cook 1987, Nordstrom 1987, Baker 1990, Iconomou 1993, Neale 1988, Buhrer 1988, Marks 1987, Sharpe 1987). It has made it possible to cover even wider defects with neighboring skin (Radovan 1984). Relative to other reconstructive options, donor site morbidity is minor and aesthetic results are reported to be improved (Iconomou 1993). The authors present a case of a patient who suffered from third-degree flame burns to the face. Primarily, the patient was treated with skin-grafting procedures leaving him with severe scar deformity of the face. The patient was treated utilizing multiple tissue expansion. A 30 year old man suffered third-degree flame burns to the face and chest following a fire accident. Prior skin grafting procedures left him with severe scar deformity of the face. Two 500 ml expanders were used, in the cheek region of either side. The expanders were inserted into the normal skin adjacent to the burned area. The ports were placed in separate pockets. The patient received peri-operative anti- biotic. Expansion began intra-ope- raflvely and continued at a weekly rate. Once full expansion was achieved, the expanders were left in situ for a month before removal and transposition of the flaps. We did not have port or expander extru- sion, cellulites, flap necrosis, infec- tion, wound dehiscence, haemato- ma, leakage or superficial skin damage. No paralysis of any facial nerve branch was observed. The burn scar contractures and hypertrophic scars were excised. Large, full-thickness skin grafts were developed from relatively small donor sites using the tissue expanDers. They behaved similarly to unexpanded full-thickness skin grafts. The tissue expander-enhanced transposition flaps appeared to have enhanced vascularity and provided ample, suitable tissue for reconstruction of the face. Tissue expansion resulted in very mobile, thin, hearty flaps that provided exceptional matched skin cover for the face. In a second stage, two croissant expanders of 500 ml were used in the scalp, in a same approach for hair reconstruction. In a third stage an upper lip and nose reconstruction were achieved. With cosmetic camouflage, an excellent aesthetic result was achieved and the patient is now able to return to his former career.
DISCUSSION Burn scars often distort and restrict the mobile features of the head (Neale 1988). Patients with such a facial disfigurement present a considerable challenge to the Plastic Surgeons. To achieve an adequate functional outcome and an improvement in appearance, a large amount of soft tissue is needed. Full-thickness skin grafts and distant flaps are the usual method of coverage of facial defects, although certain small lesions can be repaired successfully with local flaps (Feldman 1990). However, the desired results are usually not achieved because of differences in the transplanted tissue, and there is often considerable morbidity at the donor sites. The use of microvascular free-tissue transfer as a tool in secondary facial burn reconstruction has not achieved the widespread acceptance it has in other surgical procedures, such as in breast surgery (Shaw 1992) and in head and neck cancer surgery (Hidalgo 1991, Shenaq 1992). Microvascular free-tissue transfer in aesthetic restoration of the burned face has been criticized for abnormal colour match, bulkiness and masking of facial expressivity (Feldman 1990). Since Radovan's 1982 landmark work on the clinical use of tissue expanders, many plastic surgeons reported their experience in facial tissue expansion (Wieslander 1991, Spence 1992, Zxllweger 1991, Neale 1993, Foyatier 1993, Foyatier 2001). Takushima et al (Takushima 2002) described the expanded Latissimus Dorsi free flap for the treatment of extensive post-burn neck contracture. Woo and Seul reported the pre-expanded arterialized venous flaps as another option for face and neck reconstruction (Woo 2001). The expansion technique is great help in improving the shape of scars using the expanding skin as full-thickness grafts. The method has been proved to have many advantages and can be widely applied. Tissue expansion better enables us to repair facial defects with supplying ideal tissue with less donor site morbidity (Fan 1991, Manders 1984, Nordstrom 1996, Radovan 1984, Toth 1990, Wieslander 1991). Tissue expansion can provide an ample, thin, well-vascularized and colour-matched flap for facial reconstruction. Furthermore, tissue expansion is considered a form of the delay phenomenon (Mitt 1976). The delay leads to improved vascularity of the expanded flap which translates to a safer, more robust flap for transposition (Taylor 1992, Cherry 1983). In our case report, the patient is a young man and has three decades of productivity; the head region was successfully reconstructed after excision of the post-burn contractures. Facial integrity has been aesthetically restored and appea rance with make-up is near normal in social settings and at conversational distances. Facial animation has been excellent, with improved, pliable soft-tissue cover over mimetic muscles of expression. The expanded facial flap is aesthetically advantageous for reconstruction of a face defect because it can cover the defect as an aesthetic unit. Tissue expanders are inserted when the burned scars (usually split skin graft) are mature, which is usually at least one year after the burn incident. A number of caveats must be met in order to achieve successful expansion (Iconomou 1993, Zoltie 1990, Azzolini 1992). The incisions should be chosen along the cleavage lines or in the inconspicuous area, such as the nasolabial fold and submandibular region. The optimal location of the valve is a "quiet" area above or lateral to (or both) the expander, and at least 7cm away. Mathematical formulae are insufficient in predicting available flap length, as elasticity and contractibility depend on individual factors. In our opinion, the expanded pocket must be longer and wider than the size of the expander base. The pocket must be closed in two layers. Peri-operative antibiotics are routine. The expander is filled on the operative table with 10% of the expander volume. This reduces the need for drains by preventing haematoma and seroma formulation, and reduces the formation of expander envelope folds. We then wait for at least one-two weeks before beginning formal expansion. We always allow a month to elapse after full expansion has been achieved, before removing the expander and inserting the flap. Overexpansion by 30-50% makes the procedure more predictable. Overexpansion is necessary to advance unburned skin flaps with not creating scar widening, lip and eyelid ectropion. To prevent deformities caused by relapse of the expanded flap, it is essential that the flap be expanded sufficiently to cover the affected site without tension. If there is severe tension when the flap is sutured, the use of a free skin graft is recommended. For eyelid ectropion, facial suspension is also effective. The deep burns of the face are a difficult problem in Plastic Surgery. They can lead to horrible scars, functionally and aesthetically. In a society focused on beauty, patients with less visible disfigurement have higher self-esteem (Lerner 1974) and can re-socialize more effective- ly wit peers and members of the opposite sex (Berscheid 1982). Tissue expansion is not a substitute for the conventional methods but rather supplemental to them. It is a useful method of achieving reconstruction of the head and neck in the burned patient. Antonyshyn 1988 Azzolini1992 Baker 1990 Berscheid 1982 Buhrer 1988 Cherry 1983 Cook 1987 Demling 1989 Fan 1991 Feldman 1987 Feldman, S.S.: Facial resurfacing: The single sheet concept. In B. Brent (Ed.), The Artistry of Plastic Surgery. St Louis: Mosby, 1987. Feldman 1990 Foyatier 1993 Foyatier 2001 Hidalgo 1991 Iconomou 1993 Lerner 1974 Manders 1984 Marks 1987 Masser 1990 Mitz 1976 Neale 1988 Neale 1993 Nordstrom 1987 Nordstrom 1996 Radovan 1984 Sharpe 1987 Shaw 1992 Shenaq 1992 Spence 1992 Takushima 2002 Taylor 1992 Toth 1990 Wieslander 1991 Woo 2001 Zellweger 1991 Zoltie 1990 |