SEPSIS IN MAJOR BURNS CASE PRESENTATION Burn is a disease with predictable evolution and adequate intensive care treatment and surgical interventions, even if complications are present, can have favorable results even if large skin surface is burned. The burn is a particular lesion which should always be considered serious; it affects the entire organism. The local lesion and the general reaction of the organism are dynamic and recognize characteristic sequences, which can be anticipated and prevented in order to minimize the complication risk and assure a vital, functional and esthetic prognosis as good as possible. The burned wound is potentially infectious; wound contamination could be present from the first hours/days (predominantly Gram +); from the 2řd week post burn the wound progressively becomes contaminated with Pseudomonas and later with Gram -. The longer the duration of conservative treatment in deep and full thickness burns, the most probable is infection starting from the burned wound and the harder it is stopped. Early excision and grafting splits this vicious circle and prevents the immunodepression. If the microorganisms from the burned wound invade the unaffected tissues, local sepsis develops; through lymphatic and vascular dissemination, systemic sepsis develops. Early recognition of local suprainfection is often difficult, considering the complexity of the wound as well as systemic clinical signs generated by metabolic, hormonal and systemic inflammatory reactions present in major burns even though sepsis is absent. Local signs of infection, at the burned wound are:
Clinical and laboratory signs suggestive for systemic sepsis:
Unfortunately, uncotrollable systemic sepsis is the most frequent cause of death in medium/major burns, even in centers with optim technical endowment. In the presence of these local or systemic signs, systemic, aggressive, wide spectrum antibiotics is instituted before bacteriologic confirmation. The prevention and treatment of septic complications for major burns patients is based on correct burn wound treatment, on rigorous application of therapeutic protocols for severe infections, on general actions for intensive care, as well as compulsive respecting the details during the entire treatment. This year in our burn unit, approximately 250 cases with major burns exceeding 20% T.B.S.A. were treated; 60 of these exceeded 40% T.B.S.A. Most of them are partial deep and deep because of lack of proper first aid and the increase of flame burns frequency. Out of 250 cases of major burns treated this year, sepsis was encountered in one patient, we analyse in this article: Patient F.T.,
Emergency treatment:
Locally the burned wounds which are deep and without tendency to spontaneous healing, are covered with dressings. Blood products are administered to correct hematologic constants. After deshocking, when the general state allows, in the 18 th day after burn, under general anesthesia, eschars tangential excision (both superior limbs, approximately 10% T.B.S.A.) and covering with skin grafts harvested from inferior limbs. Antibiotic therapy: Ticnam (Meronem) 1,5g/day and Amikactm 200mg/day. Complication: the third day after grafting septic shock develops.
Treatment Antibiotic therapy adds: Ufexil (Ciprofloxacin) 400mg/day and Targocid 400mg/day; Tienam daily dose is increased to 3g/day. Albumin and octagam are administered as well as packed red cells, platelet concentrates, fresh frozen plasma, according to laboratory findings. Under general anesthesia, antiseptic dressings with silver sulpha diazine are applied twice a day after sterilizing the wounds with betadi nc and clorhexidine. After local and general treatment:
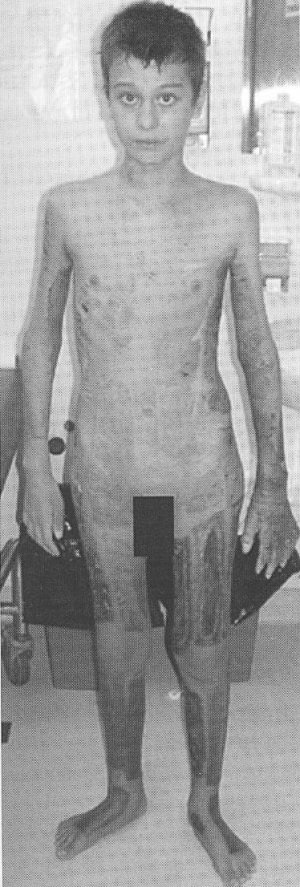
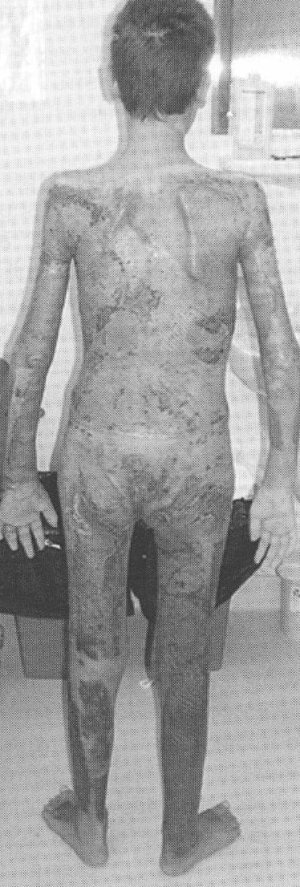
After general state stabilization, der general anesthesia, serial exsion of restant, necrotic and inted zones, resulted from graft lyis and restant eschars was perfored in 4 sessions at 7-10 days, llowed by grafting with meshed 1:1,5 split-thickness skin. Each intervention was followed by general state improvement, without any relapse. Graft integration was over 90%. Part of donor zones epithelised (approximately 30%). Local evolution was favorable with graft integration and donor zone epithelisation. In day 92 after burn, the patient is discharged with good general state, cardio-vas culary, respiratory, digestive equilibrated, afebrile. Thoughout hospitalization, according to general state, the patient benefits from kinetotherapy rehabilitation for grafted segments functionality.
Case particularities are represented by the following facts. Early surgical intervention could not be performed because the treatment in our center began 4 hours after the accident, the postcombustional shock was profound and with a long evolution, the response to therapy was slow, not allowing an early excision, we usually perform in the first 72 hours. The first excision was performed in a delicate period regarding immunologic and metabolic considerations just before granular tissue formation, at a perod of very low resources of the organism. Thus, surgical intervention timing was unusual. In day 20 post burn the burned patient suddenly develops sepsis with donor zones deepening and appearance of brown-black eschars and grafts lysing, resulting in increasing burned area from 55% to 70% T.B.S.A., lengthening the duration of the treatment with at least 1,5 months. Delaying intervention is hazardous. Of paramount importance emerges the timing of the surgical intervention for burns; it has to be thouroughly respected. The best initial intensive care is needed as well as all through hospitalization, in order to allow the surgical sequences at optimum times. Under complex antibiotic therapy (aggressive, wide spectrum) and intensive care re-equilibration, the patient overcomes the septic shock state, the excision grafting sequence was started again, this time for a considerably larger surface, finally all therapeutical efforts leading to a favorable result. Surgical sequence after complication started with left superior limb once again, in order to remove the lysed grafts and necrotic tissue. As a conclusion, burn is a disease with predictable evolution, and adequate treatment of reequilibration and surgical interventions, even if complications are present, can have favourable results even at large burned surfaces. We saw this case as an example of deshocking for a patient with major complications, who eventually lived. A burn case should never be abandoned and considered lost. Dan Enescu, Mihaela Enescu - "Arsurile copilului", Ed. Medicart, 2003 Dan Enescu, Ion Bordeianu - Manual de Chirurgie Plastica (Ovidius University Press, 2001) Principii de chirurgie plastica si microchirurgie reconstructiva, sub redactia Prof. Dr. loan Lascar, Editura National, 2005 Barret, JP, et al - Selective decontamination of the digestive tract in severely burned pediatric patients, Burns 2001 Boswick, JA Jr.- The Art and Science of Burn Care, Aspen, 1987. Carvajal, MF, Parks, DH - Burns in Children, Medical Publishers, 1988. Chaterjee, SN - Infections in Burn Patients, HER, 2000. Mabrouk AWR, - Forty years of experience in the management of the burn injuries in Egipt, HER, 2000. Pruitt, BA, et al.- Burn wound infections, World J Surg, 1998. Herndon,DN, - Total Burn Care, Saunders, 1996. |